The freezing of biological tissue is a critical concept in various fields, including medicine, cryobiology, and food science, as it directly impacts cell viability, preservation techniques, and therapeutic applications. Understanding the temperature at which tissue freezes is essential, as it typically occurs between -1°C and -5°C (30°F to 23°F), depending on factors such as tissue type, water content, and the presence of cryoprotectants. Below this range, ice crystals form within and between cells, potentially causing irreversible damage if not managed properly, while controlled freezing techniques, like vitrification, aim to minimize such harm by preventing ice crystal formation altogether.
| Characteristics | Values |
|---|---|
| Freezing Temperature of Tissue | Typically between -2°C to -5°C (28°F to 23°F) for initial ice crystal formation |
| Optimal Cryopreservation Temperature | -130°C to -196°C (-202°F to -320°F) (using liquid nitrogen) for long-term storage |
| Glass Transition Temperature | Around -120°C to -135°C (-184°F to -211°F) for water in cells |
| Lethal Temperature for Cells | Below -40°C (-40°F) due to intracellular ice formation |
| Cooling Rate for Cryopreservation | 1°C to 10°C per minute to minimize damage from ice crystal formation |
| Warming Rate for Thawing | 1°C to 5°C per minute to prevent thermal shock and recrystallization |
| Critical Factors for Freezing | Cooling rate, cryoprotectant use, and temperature uniformity |
| Cryoprotectants Used | Glycerol, DMSO, ethylene glycol, and others to reduce ice damage |
| Tissue Viability Post-Thaw | Depends on freezing method, cooling rate, and cryoprotectant efficacy |
| Applications | Organ preservation, stem cell storage, and fertility treatments |
Explore related products

$14.24 $17.99





What You'll Learn
- Cellular Damage Mechanisms: How freezing temperatures disrupt cell membranes and intracellular structures, leading to tissue injury
- Freezing Point of Tissues: Varies by tissue type due to water content and composition differences
- Cryopreservation Techniques: Methods to freeze tissues without causing irreversible damage, like vitrification
- Frostbite Pathophysiology: How prolonged cold exposure leads to tissue freezing and subsequent necrosis
- Temperature Thresholds: Specific temperatures at which different tissues begin to freeze and sustain damage
![]()
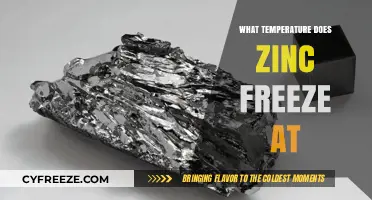
Cellular Damage Mechanisms: How freezing temperatures disrupt cell membranes and intracellular structures, leading to tissue injury
Freezing temperatures inflict cellular damage through a cascade of events that begin with the disruption of cell membranes. As temperatures drop below the freezing point of water (0°C or 32°F), extracellular fluid crystallizes into ice, drawing water out of cells through osmosis. This dehydration causes cells to shrink, increasing the concentration of solutes and straining the lipid bilayer. The membrane, once fluid and flexible, becomes rigid and brittle, losing its integrity. This mechanical stress leads to the formation of microscopic tears, allowing ions and molecules to leak in and out uncontrollably, disrupting the cell’s electrochemical balance.
Intracellular structures are equally vulnerable to freezing temperatures. Organelles like mitochondria, endoplasmic reticulum, and lysosomes are suspended in the cytosol, which also undergoes dehydration as water is drawn into extracellular ice crystals. This concentration of solutes disrupts enzymatic activity and protein folding, impairing essential metabolic processes. For example, mitochondria, the cell’s energy factories, lose their ability to produce ATP, leading to energy depletion. Additionally, ice crystals forming within the cell can physically damage organelles, further compromising cellular function.
The extent of tissue injury depends on the rate of freezing and the tissue’s water content. Slow freezing allows extracellular ice formation, which is less damaging but still dehydrates cells. Rapid freezing, on the other hand, can lead to intracellular ice formation, causing direct mechanical damage to cell membranes and organelles. Tissues with high water content, such as muscle and liver, are particularly susceptible. For instance, skin exposed to temperatures below -2°C (28.4°F) for prolonged periods can suffer frostbite, where ice crystals form in the extracellular space, leading to cell death and tissue necrosis.
Practical precautions can mitigate freezing-induced cellular damage. For cryopreservation of cells or tissues, controlled cooling rates (1°C per minute) and the use of cryoprotectants like glycerol or dimethyl sulfoxide (DMSO) are essential. These agents reduce ice crystal formation and stabilize cell membranes. In clinical settings, rewarming frozen tissues must be gradual to prevent thermal shock and further damage. For individuals exposed to extreme cold, protective measures such as insulated clothing and limiting exposure time are critical. Understanding these mechanisms not only aids in preserving biological samples but also informs strategies to prevent cold-related injuries in humans.
Above Freezing Yet Icy: Exploring How Ice Forms in Warmer Temperatures
You may want to see also
Explore related products






![]()
Freezing Point of Tissues: Varies by tissue type due to water content and composition differences
Tissue freezing is not a one-size-fits-all process. The temperature at which tissues freeze varies significantly depending on their water content and composition. For instance, adipose tissue (fat) has a lower freezing point compared to muscle tissue due to its higher lipid content, which freezes at around -1°C to -5°C. In contrast, muscle tissue, with its higher water content, typically freezes at temperatures closer to 0°C. This variability is critical in medical and scientific applications, such as cryopreservation, where understanding these differences ensures tissue viability and function post-thaw.
Consider the practical implications in cryosurgery, where extreme cold is used to destroy abnormal tissues. For skin lesions, temperatures as low as -20°C to -40°C are applied for 20–30 seconds to ensure complete destruction of the targeted tissue. However, surrounding healthy tissues, such as muscle or nerve, may have different freezing thresholds, necessitating precise control to avoid collateral damage. Clinicians must account for these differences to optimize treatment efficacy while minimizing harm.
From a preservation perspective, the freezing point of tissues directly impacts their storage and transportation. Organs like the liver, with a water content of approximately 70%, require careful cooling to just below 0°C to prevent ice crystal formation, which can rupture cell membranes. In contrast, bone marrow, with its denser composition, can tolerate slightly lower temperatures without significant damage. Cryoprotectants, such as glycerol or dimethyl sulfoxide (DMSO), are often used to lower the freezing point and protect tissues during the freezing process, but their effectiveness varies by tissue type.
A comparative analysis reveals that tissues with higher salt and protein content, like cartilage, freeze at lower temperatures due to their ability to depress the freezing point of water. This phenomenon, known as freezing point depression, is analogous to adding salt to ice to lower its melting point. However, tissues with higher lipid content, such as brain tissue, exhibit a more complex freezing behavior due to the phase transitions of fats. Understanding these nuances is essential for developing tailored cryopreservation protocols that preserve tissue integrity across diverse types.
In summary, the freezing point of tissues is not uniform but rather a function of their unique water content and composition. This variability demands a nuanced approach in both medical treatments and preservation techniques. By accounting for these differences, practitioners can enhance outcomes, whether in cryosurgery, organ transplantation, or tissue banking. Practical tips include using tissue-specific cryoprotectants, monitoring cooling rates, and employing advanced imaging techniques to assess ice formation in real time. Such precision ensures that the benefits of freezing are maximized while risks are minimized.
Surviving Extreme Cold: Essential Tips for Below-Freezing Temperatures
You may want to see also
Explore related products





![]()
Cryopreservation Techniques: Methods to freeze tissues without causing irreversible damage, like vitrification
Tissue freezing is a delicate balance between preserving cellular integrity and preventing ice crystal formation, which can rupture cell membranes. Cryopreservation techniques aim to achieve this by manipulating temperature, cooling rates, and cryoprotectant solutions. Among these methods, vitrification stands out as a transformative approach, offering a way to freeze tissues without the damaging effects of ice crystallization.
Vitrification involves transforming a tissue into a glass-like state rather than a crystalline structure. This is achieved by using high concentrations of cryoprotective agents (CPAs) such as glycerol, ethylene glycol, or dimethyl sulfoxide (DMSO), which depress the freezing point and increase viscosity, preventing ice formation. For example, in oocyte cryopreservation, a common CPA mixture includes 15% ethylene glycol and 15% DMSO, combined with a slow cooling protocol to reach temperatures as low as -196°C (the boiling point of liquid nitrogen). The key is to cool the tissue rapidly enough to avoid ice crystal formation but not so fast as to cause mechanical damage.
While vitrification is highly effective, it is not without challenges. High CPA concentrations can be toxic to cells, necessitating precise timing and controlled exposure. For instance, exposure to 2 M DMSO for more than 20 minutes can reduce cell viability in some tissues. To mitigate this, stepwise CPA addition and removal protocols are employed, often involving equilibration steps where tissues are gradually exposed to increasing CPA concentrations. Additionally, warming must be equally controlled to prevent devitrification, where the glass-like state reverts to a crystalline one, causing damage.
Comparatively, slow freezing methods, which cool tissues at rates of 1–10°C per minute, rely on controlled ice formation in extracellular spaces while using lower CPA concentrations. However, this approach often results in intracellular ice formation at temperatures below -40°C, making it less suitable for complex tissues. Vitrification, on the other hand, bypasses this issue entirely, making it ideal for organs, embryos, and other delicate tissues. Its success hinges on meticulous protocol adherence, from CPA selection to cooling and warming rates.
In practice, vitrification has revolutionized fields like reproductive medicine, where it enables the long-term storage of oocytes and embryos with survival rates exceeding 90%. For researchers and clinicians, adopting vitrification requires access to specialized equipment, such as high-precision freezers and liquid nitrogen storage, as well as training in handling CPAs. While the technique demands expertise, its ability to preserve tissues without irreversible damage makes it an indispensable tool in cryobiology.
Perfect Sorbet Texture: Ideal Freezer Temperature Tips for Homemade Treats
You may want to see also
Explore related products






![]()
Frostbite Pathophysiology: How prolonged cold exposure leads to tissue freezing and subsequent necrosis
Tissue freezing occurs at temperatures below -0.5°C (31.1°F), the point at which intracellular water begins to crystallize. This threshold is critical in understanding frostbite pathophysiology, as prolonged exposure to extreme cold triggers a cascade of cellular damage. When skin and subcutaneous tissues are subjected to temperatures between -2°C and -15°C (28.4°F to 5°F), ice crystals form extracellularly, drawing water out of cells and causing dehydration. This osmotic shift leads to cellular shrinkage, membrane rupture, and eventual necrosis. Notably, extremities like fingers, toes, ears, and nose are most vulnerable due to their distal location and reduced blood flow, which limits heat retention.
The progression of frostbite is staged, with each phase reflecting escalating tissue damage. In the first stage (frostnip), skin appears pale and numb but remains pliable, with no permanent damage. The second stage (superficial frostbite) involves ice crystal formation in the epidermis and dermis, causing blistering upon rewarming. The third stage (deep frostbite) extends to subcutaneous tissues, muscles, and tendons, leading to tissue death and potential autoamputation. Critical to this process is the role of vasoconstriction, which reduces blood flow to conserve core temperature but starves peripheral tissues of oxygen and nutrients, exacerbating ischemia-reperfusion injury.
Rewarming, while essential, must be managed carefully to minimize further damage. Thawing frozen tissue at 37°C to 40°C (98.6°F to 104°F) using warm water or heating blankets is recommended, but rapid temperature changes can cause thermal shock. Avoid rubbing or massaging affected areas, as this can disrupt fragile blood vessels and worsen tissue injury. Pain management with NSAIDs or opioids is often necessary, as rewarming triggers intense pain due to nerve activation. For severe cases, thrombolytic therapy or surgical debridement may be required to prevent gangrene.
Prevention remains the most effective strategy, particularly for individuals at high risk, such as outdoor workers, mountaineers, and military personnel. Wearing moisture-wicking layers, insulated footwear, and windproof outerwear can maintain skin temperature. Limiting exposure to temperatures below -15°C (5°F) and wind chills below -28°C (-18°F) is crucial, as wind accelerates heat loss. Recognizing early signs of frostnip—such as tingling, numbness, or skin whitening—allows for prompt intervention, like seeking warmth or using chemical warmers. Education on cold weather safety and immediate rewarming techniques can significantly reduce the incidence and severity of frostbite.
Understanding the pathophysiology of frostbite underscores the importance of timely intervention and preventive measures. While tissue freezing begins at -0.5°C, the cumulative effects of cold exposure, vasoconstriction, and ischemia drive irreversible damage. By addressing both the physiological mechanisms and practical strategies, individuals can mitigate risks and protect against this debilitating condition. Whether through proper attire, environmental awareness, or emergency response, proactive steps are key to preserving tissue viability in extreme cold.
Lauric Acid's Freezing and Melting Point: Same Temperature Explained
You may want to see also
Explore related products






![]()
Temperature Thresholds: Specific temperatures at which different tissues begin to freeze and sustain damage
Tissue freezing is not a one-size-fits-all phenomenon. Different tissues exhibit varying susceptibility to cold injury, with critical temperature thresholds dictating when cellular damage begins. Skin, for instance, starts to freeze at around -0.5°C to -1.5°C (31°F to 29.3°F), leading to frostnip—a superficial, reversible injury. However, deeper tissues like muscle and internal organs are more resilient, typically sustaining damage at temperatures below -2°C to -3°C (28.4°F to 26.6°F). Understanding these thresholds is crucial for medical applications, such as cryosurgery, where controlled freezing is used to destroy abnormal tissues while sparing healthy ones.
In cryopreservation, the process of preserving cells, tissues, or organs by cooling, the temperature threshold is even more critical. For example, sperm and embryos can be successfully frozen at temperatures around -196°C (-320.8°F) using liquid nitrogen, with minimal damage due to their small size and high surface-area-to-volume ratio. In contrast, larger tissues like organs face challenges due to ice crystal formation, which occurs between 0°C and -5°C (32°F to 23°F). These crystals can puncture cell membranes, leading to irreversible damage. Techniques like vitrification, which cools tissues rapidly to avoid ice formation, are employed to bypass this threshold, but they require precise control and specialized solutions.
Age and health status significantly influence tissue freezing thresholds. Children and the elderly are more susceptible to cold injuries due to reduced circulation and thinner subcutaneous fat layers. For instance, a child’s skin may freeze at slightly higher temperatures than an adult’s, making them more vulnerable to frostbite in cold environments. Similarly, individuals with conditions like diabetes or Raynaud’s disease experience impaired blood flow, lowering their tissue freezing threshold. Practical precautions, such as wearing insulated clothing and limiting exposure to extreme cold, are essential for at-risk populations.
In clinical settings, understanding temperature thresholds is vital for procedures like cryoablation, where freezing is used to destroy tumors. For example, prostate cancer treatment often involves freezing tissue to temperatures between -40°C and -60°C (-40°F to -76°F) to ensure complete tumor destruction. However, adjacent healthy tissues must be protected, as they can sustain damage at temperatures below -3°C (26.6°F). Cryoprotectants and ultrasound monitoring are used to mitigate risks, highlighting the importance of precision in temperature control. This knowledge not only improves treatment efficacy but also minimizes complications, ensuring patient safety.
Finally, environmental exposure to freezing temperatures demands awareness of tissue thresholds for prevention. Frostbite, a common cold injury, progresses in stages, with skin turning pale and numb at -2°C to -3°C (28.4°F to 26.6°F). At temperatures below -10°C (14°F), deeper tissues like muscle and bone can be affected, leading to permanent damage. Immediate rewarming in warm water (40°C to 42°C or 104°F to 107.6°F) is critical, but rubbing the affected area should be avoided to prevent further tissue injury. By recognizing these thresholds, individuals can take proactive measures to protect themselves in cold environments, reducing the risk of severe cold-related injuries.
Understanding Domestic Gas Freezing Point: Temperature Threshold Explained
You may want to see also
Frequently asked questions
Tissue typically begins to freeze at temperatures around -0.5°C to -1.5°C (31°F to 29.2°F), depending on the tissue type and its water content.
Yes, freezing tissue can cause permanent damage due to ice crystal formation, which disrupts cell membranes and structures, leading to cell death.
Skin tissue can begin to freeze at temperatures below -0.5°C (31°F), but the risk of frostbite increases significantly at temperatures below -15°C (5°F).
Yes, tissue can be preserved using cryoprotectants and controlled freezing techniques (e.g., vitrification) to minimize ice crystal damage and maintain viability.
Human tissue is typically cryopreserved at temperatures below -130°C (-202°F) in liquid nitrogen to prevent ice crystal formation and preserve cellular integrity.