Dermatologists commonly use a procedure called cryotherapy to freeze and destroy skin cancer cells. This minimally invasive technique involves applying extremely cold temperatures, typically with liquid nitrogen, to the affected area, which causes the cancerous tissue to freeze, thaw, and eventually slough off. Cryotherapy is particularly effective for treating superficial skin cancers like basal cell carcinoma and actinic keratosis, as well as precancerous lesions. The procedure is quick, often performed in-office, and generally well-tolerated, though it may cause temporary side effects such as redness, blistering, or scarring. Its precision and effectiveness make it a popular choice for early-stage skin cancer treatment.
| Characteristics | Values |
|---|---|
| Procedure Name | Cryotherapy |
| Primary Agent Used | Liquid Nitrogen |
| Temperature Range | -196°C (-320°F) |
| Application Method | Spray, Cotton Swab, or Cryoprobe |
| Targeted Skin Cancers | Actinic Keratosis, Basal Cell Carcinoma, Squamous Cell Carcinoma (early stages) |
| Mechanism of Action | Freezes and destroys cancerous cells by forming ice crystals |
| Duration of Treatment | 5–10 seconds per lesion (may vary) |
| Number of Sessions | 1–3 sessions, depending on severity |
| Healing Time | 1–4 weeks (blistering, scabbing, and peeling may occur) |
| Side Effects | Pain, redness, swelling, blistering, scarring (rare), hypopigmentation |
| Success Rate | 70–90% for eligible lesions |
| Contraindications | Cold intolerance, cryoglobulinemia, Raynaud’s disease, large or deep tumors |
| Post-Treatment Care | Keep area clean, avoid picking scabs, use sunscreen |
| Alternative Treatments | Surgical excision, Mohs surgery, topical chemotherapy, laser therapy |
| Cost Range (USA) | $100–$500 per session (varies by location and insurance) |
| FDA Approval | Approved for actinic keratosis and certain skin cancers |
| Latest Advances | Precision cryosprays, real-time temperature monitoring devices |
Explore related products






What You'll Learn
![]()
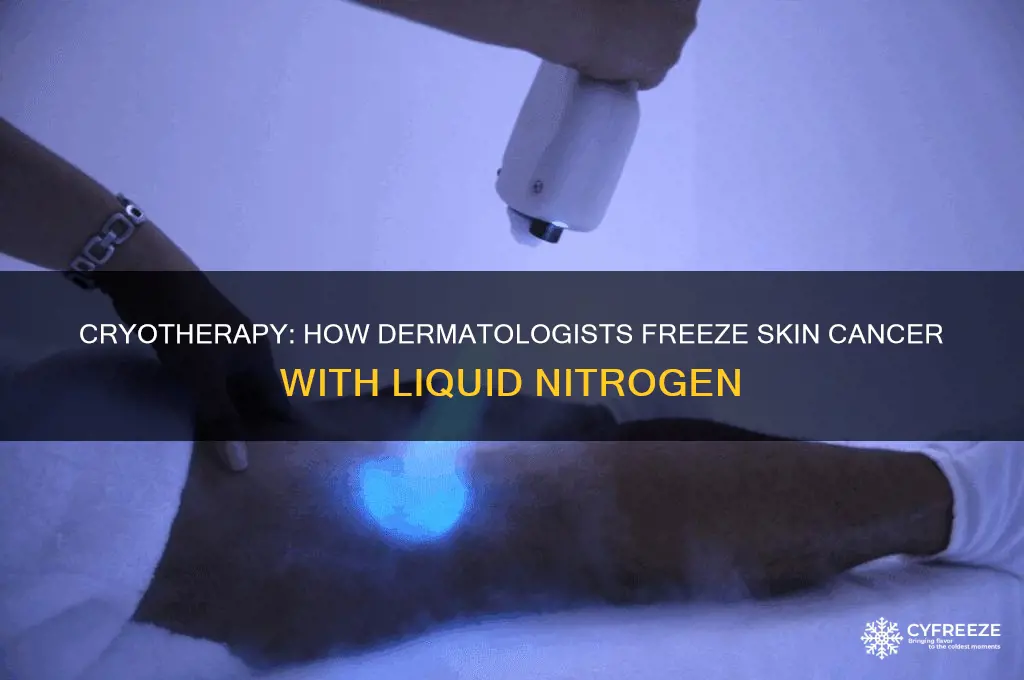
Cryotherapy with liquid nitrogen
Liquid nitrogen, with its chilling temperature of -196°C (-320°F), is a dermatologist's precision weapon against certain skin cancers and precancerous lesions. This cryotherapy technique leverages extreme cold to destroy abnormal cells by freezing them, causing ice crystals to form within the cells, disrupting their structure, and leading to cell death. The procedure is particularly effective for superficial skin cancers like basal cell carcinoma, squamous cell carcinoma in situ (Bowen's disease), and actinic keratosis, a common precancerous condition.
Its application is straightforward yet requires skill. The dermatologist uses a cryoprobe or cotton-tipped applicator to apply liquid nitrogen directly to the lesion. The freezing time varies depending on the lesion type and size, typically ranging from 5 to 30 seconds. A freezing time of 20-30 seconds, followed by a thawing period, is often repeated in cycles to ensure complete destruction of the targeted tissue. This method is favored for its simplicity, minimal scarring, and high success rates, especially for early-stage cancers.
While cryotherapy with liquid nitrogen is generally safe, it's not without considerations. Patients may experience temporary side effects such as redness, swelling, blistering, and discomfort at the treatment site. In rare cases, hypopigmentation (lightening of the skin) or scarring can occur. It's crucial for patients to follow post-treatment care instructions, including keeping the treated area clean and protected from the sun, to minimize these risks. This treatment is typically not recommended for large or deep lesions, as the freezing effect may not penetrate sufficiently to destroy all cancerous cells.
The appeal of cryotherapy lies in its non-invasiveness and convenience. Unlike surgical excision, it doesn't require stitches and has a shorter recovery time. However, its effectiveness is highly dependent on the expertise of the dermatologist in determining the appropriate freezing time and technique. For optimal outcomes, patients should seek treatment from experienced dermatologists who can tailor the procedure to the specific characteristics of the lesion and the patient's skin type.
In conclusion, cryotherapy with liquid nitrogen stands as a valuable tool in the dermatologist's arsenal for treating skin cancer. Its precision, efficacy, and minimal downtime make it a preferred option for eligible patients. However, the success of the treatment hinges on accurate diagnosis, proper technique, and patient compliance with aftercare instructions. As with any medical procedure, a thorough consultation with a qualified dermatologist is essential to determine if cryotherapy is the right choice for an individual's specific condition.
Is Max Freeze Safe for Pregnant Women? Expert Advice
You may want to see also
Explore related products






![]()
Precancerous lesion removal techniques
Dermatologists often employ cryotherapy as a primary method to treat precancerous lesions, such as actinic keratosis (AK), which are rough, scaly patches caused by sun damage. This technique involves applying liquid nitrogen, at a temperature of -196°C (-320°F), directly to the lesion using a spray device or cotton-tipped applicator. The extreme cold destroys the abnormal cells by causing intracellular ice formation and vascular stasis, effectively "freezing" the lesion. Cryotherapy is particularly favored for its simplicity, minimal invasiveness, and high success rate, typically ranging from 70% to 90% for AKs. However, multiple sessions may be required, and the procedure can cause temporary side effects like blistering, scarring, or hypopigmentation.
For patients seeking alternatives to cryotherapy, curettage and electrodessication (C&D) is a widely used technique. This two-step process begins with curettage, where the dermatologist scrapes away the lesion using a sharp, ring-shaped instrument called a curette. Electrodessication follows, applying an electric current to the area to cauterize remaining abnormal cells and stop bleeding. C&D is highly effective for precancerous lesions, with cure rates exceeding 95%, and it allows for precise tissue removal. However, it may leave a small scar, making it less ideal for cosmetically sensitive areas like the face. This method is often recommended for thicker or more persistent lesions that cryotherapy cannot fully address.
Another emerging technique is topical field therapy, which targets not only visible lesions but also subclinical lesions in the surrounding area. This approach uses medications like 5-fluorouracil (5-FU) or imiquimod, applied directly to the skin for several weeks. 5-FU acts as a chemotherapy agent, disrupting abnormal cell growth, while imiquimod stimulates the immune system to attack precancerous cells. These treatments are particularly useful for patients with widespread actinic damage or multiple lesions. Side effects, such as redness, crusting, and irritation, can be intense but are generally temporary. Topical field therapy is a proactive strategy, reducing the risk of future skin cancers by addressing both visible and invisible precancerous changes.
Laser therapy, specifically using devices like the carbon dioxide (CO2) laser or pulsed-dye laser, offers a precise and controlled method for removing precancerous lesions. The CO2 laser vaporizes tissue with a focused beam of light, effectively destroying abnormal cells while minimizing damage to surrounding skin. Pulsed-dye lasers target blood vessels within the lesion, disrupting their supply and causing cell death. Laser therapy is particularly advantageous for its precision, making it suitable for delicate areas like the face. However, it can be more expensive and may require specialized equipment and expertise. Recovery time varies, with potential side effects including redness, swelling, and temporary discoloration.
Finally, photodynamic therapy (PDT) is a two-step procedure that combines a photosensitizing agent with light activation to destroy precancerous cells. The patient first applies a topical solution, such as aminolevulinic acid (ALA), which is absorbed by abnormal cells. After incubation, a specific wavelength of light is directed at the area, activating the agent and producing a chemical reaction that kills the targeted cells. PDT is highly effective for actinic keratoses, with clearance rates around 80-90%, and it offers the added benefit of improving overall skin texture. However, patients must avoid sunlight for 48 hours post-treatment, as the skin remains sensitive to light. This method is particularly appealing for its cosmetic outcomes, as it typically leaves minimal scarring.
Do Dermatologists Use a Different Method to Freeze Warts?
You may want to see also
Explore related products






![]()
Freezing basal cell carcinoma
Dermatologists often employ cryotherapy as a precise and effective method to treat basal cell carcinoma (BCC), the most common form of skin cancer. This technique involves freezing the cancerous tissue with liquid nitrogen, which is applied directly to the lesion using a spray device, cotton swab, or cryoprobe. The extreme cold destroys the cancer cells by causing ice crystal formation and subsequent cell rupture, while also triggering an immune response that aids in eliminating the damaged tissue. Cryotherapy is particularly suited for superficial BCCs, as well as those located in areas where surgical excision might be cosmetically challenging, such as the face.
The procedure itself is relatively straightforward and typically performed in a dermatologist’s office. After numbing the area with a local anesthetic if necessary, the dermatologist applies liquid nitrogen at temperatures as low as -196°C (-320°F) for 10 to 30 seconds, followed by a thawing period. This freeze-thaw cycle may be repeated to ensure complete destruction of the cancerous cells. Patients often experience a mild stinging or burning sensation during the process, but it is generally well-tolerated. Post-treatment, a blister or scab forms over the treated area, which usually heals within 2 to 4 weeks, leaving minimal scarring in most cases.
While cryotherapy is effective for early-stage or superficial BCCs, it may not be the best option for deeper or more aggressive tumors. Its success rate for superficial BCCs is approximately 85-90%, but this drops for nodular or infiltrative subtypes. Dermatologists often consider factors such as the lesion’s size, location, and the patient’s overall health when deciding on cryotherapy. For instance, older adults or those with compromised immune systems may benefit from this non-invasive approach, as it avoids the risks associated with surgery.
One practical tip for patients undergoing cryotherapy is to keep the treated area clean and dry during the healing process. Applying petroleum jelly or a prescribed ointment can help soothe the skin and prevent infection. It’s also crucial to avoid picking at the scab, as this can delay healing and increase the risk of scarring. Follow-up appointments are essential to monitor the site and ensure the cancer has been fully eradicated, as recurrence is possible if any cancerous cells remain.
In comparison to other treatments like surgical excision or Mohs surgery, cryotherapy offers a less invasive option with quicker recovery times. However, it lacks the ability to confirm complete removal of cancer cells during the procedure, a key advantage of Mohs surgery. For this reason, cryotherapy is often reserved for low-risk BCCs or cases where surgery is not feasible. Patients should discuss their specific situation with a dermatologist to determine the most appropriate treatment plan, balancing efficacy, convenience, and cosmetic outcomes.
Master Freezing Beans with a Food Saver: Easy Preservation Tips
You may want to see also
Explore related products





![]()
Squamous cell carcinoma cryosurgery
Cryosurgery stands as a cornerstone in the treatment of squamous cell carcinoma (SCC), a common form of skin cancer. This minimally invasive procedure leverages extreme cold, typically from liquid nitrogen, to destroy cancerous cells. Applied directly to the lesion, the freezing temperatures cause cellular dehydration, protein denaturation, and ultimately, cell death. Dermatologists favor cryosurgery for its precision, efficacy, and minimal scarring, particularly in treating early-stage SCC on the face, ears, and scalp—areas where preserving cosmetic outcomes is crucial.
The procedure itself is straightforward yet requires skill. After cleaning the target area, the dermatologist applies liquid nitrogen, often via a spray device or cotton-tipped applicator, for 20 to 30 seconds, achieving a freeze-thaw-freeze cycle to ensure complete cell destruction. The treated area may blister, crust, or turn red, with healing typically occurring within 2 to 4 weeks. While cryosurgery is generally well-tolerated, it’s most effective for small, superficial SCCs; larger or deeper lesions may require surgical excision or other treatments.
One of the key advantages of cryosurgery is its accessibility and cost-effectiveness. It’s particularly beneficial for elderly patients or those with comorbidities who may not tolerate more invasive procedures. However, it’s not without limitations. Recurrence rates for SCC treated with cryosurgery can be higher than with surgical excision, especially for high-risk lesions. Dermatologists often recommend follow-up biopsies or imaging to confirm complete eradication of cancer cells.
Practical tips for patients undergoing cryosurgery include keeping the treated area clean and dry, avoiding sun exposure, and applying recommended topical antibiotics or dressings. While discomfort is minimal, over-the-counter pain relievers can manage any post-procedure soreness. For optimal outcomes, adherence to post-treatment care and regular skin examinations are essential to detect and address any recurrence promptly.
In comparison to other SCC treatments like Mohs surgery or radiation therapy, cryosurgery offers a balance of simplicity and effectiveness for select cases. Its non-excisional nature makes it less invasive, but it’s not a one-size-fits-all solution. Dermatologists carefully evaluate lesion size, location, and patient health before recommending cryosurgery, ensuring the chosen treatment aligns with both clinical and cosmetic goals. When used appropriately, cryosurgery remains a valuable tool in the dermatologist’s arsenal against squamous cell carcinoma.
Harmonix Freeze Pedal Compatibility with Piani: A Creative Music Setup
You may want to see also
Explore related products






![]()
Post-treatment skin care tips
Cryotherapy, a common method dermatologists use to freeze and destroy skin cancer cells, leaves the treated area vulnerable and sensitive. Post-treatment care is crucial to ensure proper healing and minimize complications. Immediately after the procedure, a blister or crust may form, which should be treated with gentle care. Avoid picking, scratching, or applying pressure to the area, as this can lead to infection or scarring. Instead, keep the site clean by washing it daily with mild soap and lukewarm water, then patting it dry with a soft towel.
Moisturizing is another critical step in post-cryotherapy care. The treated skin can become dry and irritated, so applying a fragrance-free, hypoallergenic moisturizer twice daily helps maintain the skin’s barrier function. Look for products containing ceramides or hyaluronic acid, which are particularly effective at retaining moisture. For added protection, consider using a thin layer of petroleum jelly to seal in hydration, especially if the area feels particularly tight or cracked.
Sun protection is non-negotiable after cryotherapy. The treated skin is more susceptible to UV damage, which can hinder healing and increase the risk of recurrence. Apply a broad-spectrum sunscreen with an SPF of 30 or higher every morning, even on cloudy days. Reapply every two hours if you’re outdoors, and wear protective clothing, such as wide-brimmed hats and long sleeves, to shield the area from direct sunlight. For children and adults with sensitive skin, mineral-based sunscreens containing zinc oxide or titanium dioxide are less likely to cause irritation.
Monitoring the healing process is essential to catch any signs of infection or abnormal healing early. Keep an eye on the treated area for redness, swelling, pus, or persistent pain, which could indicate an infection requiring medical attention. Additionally, if the crust or blister does not heal within 2–4 weeks, or if the skin changes color or texture unexpectedly, consult your dermatologist. Regular follow-up appointments are also recommended to ensure the treatment was successful and to address any concerns promptly.
Finally, lifestyle adjustments can significantly impact post-treatment recovery. Stay hydrated and maintain a balanced diet rich in vitamins C and E, which support skin repair. Avoid smoking and limit alcohol consumption, as both can impair healing and increase inflammation. For older adults or those with compromised immune systems, extra caution is advised, as healing may take longer and complications are more likely. By following these targeted post-treatment skin care tips, you can promote optimal healing and reduce the risk of long-term issues.
Overusing Blue Fat Freeze: Risks and Safe Application Limits Explained
You may want to see also
Frequently asked questions
Dermatologists typically use liquid nitrogen, which is extremely cold (around -196°C or -320°F), to freeze and destroy skin cancer cells in a procedure called cryotherapy.
Liquid nitrogen is applied directly to the skin cancer lesion, freezing the cells rapidly. This causes the water inside the cells to form ice crystals, which disrupts the cell membrane and leads to the destruction of the cancerous tissue.
Cryotherapy is most effective for superficial skin cancers like basal cell carcinoma and actinic keratosis. It may not be suitable for deeper or more aggressive cancers, as it primarily treats surface-level lesions. Always consult a dermatologist for the best treatment option.