When considering egg freezing, one of the critical factors evaluated is Anti-Müllerian Hormone (AMH) levels, which reflect ovarian reserve and predict the number of eggs a woman may retrieve during the process. While there is no strict cutoff, AMH levels below 1.0 ng/mL are generally considered low and may indicate a reduced ovarian reserve, potentially leading to fewer eggs retrieved during a freezing cycle. However, even with low AMH, egg freezing can still be a viable option, as individual responses to stimulation vary. It’s essential to consult with a fertility specialist who can assess your specific situation, discuss expectations, and tailor a treatment plan to maximize the chances of success.
| Characteristics | Values |
|---|---|
| Optimal AMH Level for Egg Freezing | 2.0–6.8 ng/mL (higher levels generally indicate better ovarian reserve) |
| Borderline AMH Level | 1.0–2.0 ng/mL (may still be considered for egg freezing with caution) |
| Low AMH Level | 0.5–1.0 ng/mL (reduced success rates, but egg freezing may still be attempted) |
| Very Low AMH Level | <0.5 ng/mL (significantly reduced ovarian reserve; egg freezing success is unlikely) |
| Minimum AMH Level for Consideration | Some clinics may consider levels as low as 0.3 ng/mL, but success is rare |
| Age Influence | Lower AMH levels are more common in older women (e.g., >35 years) |
| Success Rates with Low AMH | Lower AMH correlates with fewer retrieved eggs and lower live birth rates |
| Additional Factors Considered | Antral follicle count (AFC), age, and overall ovarian health |
| Recommendation | Consult a fertility specialist for personalized assessment and options |
Explore related products






What You'll Learn
![]()
AMH Levels for Egg Freezing
Anti-Müllerian hormone (AMH) serves as a critical biomarker for ovarian reserve, directly influencing decisions around egg freezing. While no universal threshold exists, AMH levels below 1.0 ng/ml often signal diminished ovarian reserve, complicating the retrieval of a viable egg count. Women in their late 30s or early 40s frequently fall into this range, but younger individuals with levels this low may require aggressive stimulation protocols or reconsideration of fertility preservation options.
Consider a 35-year-old with an AMH of 0.8 ng/ml: her cycle might yield 3–5 eggs, insufficient for multiple future attempts. Clinics often recommend retrieving eggs sooner rather than later in such cases, as AMH declines accelerate with age. Conversely, an AMH of 2.0–3.0 ng/ml (common in late 30s) typically allows for 8–12 eggs per cycle, providing a more robust safety net.
For those with AMH levels below 0.5 ng/ml, egg freezing becomes less predictable. Protocols may involve higher doses of gonadotropins (e.g., 300–450 IU daily) to stimulate follicles, though success rates drop significantly. In these scenarios, clinics often discuss adjunctive strategies like double stimulation cycles or donor egg options.
Practical steps for low-AMH candidates include prioritizing timing, opting for experienced fertility centers, and maintaining open communication about expectations. While AMH isn’t the sole determinant of egg freezing success, it remains a cornerstone for tailoring protocols and managing outcomes. Women with borderline or low levels should approach the process with urgency and realism, balancing hope with data-driven decisions.
Can You Freeze Boiled Eggs? Tips for Preserving Hard-Boiled Eggs
You may want to see also
Explore related products






![]()
Ideal AMH Range for Fertility
Anti-Müllerian hormone (AMH) levels serve as a critical marker of ovarian reserve, reflecting the number of remaining eggs. For women considering egg freezing, understanding the ideal AMH range for fertility is essential. Typically, an AMH level between 1.0 and 4.0 ng/mL is considered optimal for natural fertility. Below 1.0 ng/mL, ovarian reserve is often classified as low, signaling a diminished egg count and potentially reduced success rates with fertility treatments. However, this threshold isn’t absolute; individual factors like age, overall health, and response to stimulation play significant roles. For egg freezing, clinics often proceed with AMH levels as low as 0.7 ng/mL, though lower values may require more aggressive stimulation protocols or additional cycles to retrieve a viable number of eggs.
Analyzing AMH trends reveals a stark decline with age, making it a time-sensitive metric. Women in their early 30s with an AMH of 2.0–3.0 ng/mL may still achieve satisfactory egg retrieval outcomes, but those in their late 30s or early 40s with levels below 1.5 ng/mL face greater challenges. For instance, a 35-year-old with an AMH of 1.2 ng/mL might need higher doses of follicle-stimulating hormone (FSH) during stimulation, such as 300–450 IU daily, compared to a younger woman with higher AMH. This underscores the importance of early assessment and personalized treatment plans.
Persuasively, AMH should not be viewed in isolation. While a low AMH may prompt urgency, it doesn’t preclude successful egg freezing. Advances in fertility technology, such as individualized stimulation protocols and improved vitrification techniques, have expanded possibilities for women with diminished ovarian reserve. For example, a 40-year-old with an AMH of 0.8 ng/mL might still retrieve 5–8 mature eggs over two cycles, sufficient for potential future use. The key is proactive decision-making: women with borderline or low AMH levels (below 1.5 ng/mL) should consult a reproductive endocrinologist promptly to explore options like higher-dose medications or adjunct therapies like dehydroepiandrosterone (DHEA) supplementation.
Comparatively, AMH thresholds for egg freezing differ from those for in vitro fertilization (IVF). While IVF often requires a higher egg yield per cycle, egg freezing focuses on cumulative retrieval over multiple cycles if needed. A woman with an AMH of 0.5 ng/mL might not be an ideal IVF candidate but could still freeze eggs through extended protocols. This highlights the flexibility of egg freezing as a fertility preservation method, even for those with suboptimal AMH levels.
Practically, women considering egg freezing should monitor AMH annually starting in their early 30s, especially if they have risk factors like a family history of early menopause or prior ovarian surgery. Lifestyle modifications, such as maintaining a healthy weight and avoiding smoking, can support ovarian health but won’t reverse AMH decline. For those with low AMH, combining egg freezing with embryo banking (if partnered) may offer additional security. Ultimately, the ideal AMH range for fertility preservation is less about hitting a specific number and more about timely action and tailored strategies to maximize outcomes.
Can You Freeze Egg Roll Wrappers? A Complete Storage Guide
You may want to see also
Explore related products






![]()
Low AMH and Success Rates
Anti-Müllerian hormone (AMH) levels below 1.0 ng/ml often trigger concerns about egg freezing success rates. This threshold signals diminished ovarian reserve, but it’s not a definitive barrier. Women with AMH levels as low as 0.5 ng/ml have successfully frozen eggs, though the yield is typically lower—around 3–5 mature eggs per cycle compared to 10–15 in those with higher AMH. Clinics may recommend aggressive stimulation protocols, such as higher doses of gonadotropins (e.g., 300–450 IU daily) or adjunct medications like DHEA (75 mg daily for 3–6 months), to optimize retrieval in these cases.
The relationship between AMH and live birth rates post-thaw is nuanced. Studies show that women with AMH below 1.0 ng/ml have a 30–40% chance of live birth per thawed egg, compared to 50–60% in those with AMH above 2.0 ng/ml. However, age remains a dominant factor—a 35-year-old with low AMH may still have better outcomes than a 40-year-old with higher AMH. Embryologists often recommend preimplantation genetic testing (PGT) for embryos from low-AMH cycles to improve implantation rates, as these eggs are more likely to carry chromosomal abnormalities.
For those considering egg freezing with low AMH, timing is critical. Starting the process within 6–12 months of receiving the diagnosis maximizes the chances of retrieving viable eggs. Lifestyle modifications, such as maintaining a BMI between 18.5–24.9, reducing alcohol intake, and quitting smoking, can also improve ovarian response. Some clinics offer "mini-stim" protocols, using lower doses of medication (e.g., 150 IU gonadotropins) over multiple cycles, though this approach may extend the overall timeline.
A comparative analysis of clinics reveals that success rates for low-AMH patients vary widely—from 10% to 40% live births per thawed egg—depending on the clinic’s expertise and technology. Centers specializing in diminished ovarian reserve often employ advanced techniques like in vitro maturation (IVM) or individualized stimulation protocols based on antral follicle count. Prospective patients should inquire about a clinic’s experience with low-AMH cases and request data-driven projections rather than relying on general statistics.
Ultimately, low AMH does not preclude successful egg freezing, but it requires strategic planning and realistic expectations. Combining medical interventions with lifestyle adjustments and selecting a clinic with proven expertise in low-reserve cases can significantly improve outcomes. While the journey may be more challenging, many women with AMH levels below 1.0 ng/ml have preserved their fertility and achieved successful pregnancies through frozen eggs.
Freezing PB Mixture for PB Eggs: A Sweet Storage Solution
You may want to see also
Explore related products






![]()
AMH Testing Before Egg Freezing
Anti-Müllerian hormone (AMH) levels serve as a critical biomarker for ovarian reserve, directly influencing decisions around egg freezing. While no universal threshold dictates when to freeze eggs, AMH values below 1.0 ng/mL often signal diminished ovarian reserve, prompting urgent consideration of fertility preservation. For context, women in their 20s typically have AMH levels between 2.0–6.8 ng/mL, while those in their late 30s may drop to 0.5–3.0 ng/mL. A result below 1.0 ng/mL, particularly in women under 35, indicates a higher risk of poor egg retrieval outcomes, making AMH testing an essential first step before proceeding with egg freezing.
Interpreting AMH results requires nuance, as the hormone’s predictive power varies by age and individual health factors. For instance, a 30-year-old with an AMH of 1.5 ng/mL may still achieve a reasonable egg yield, whereas a 40-year-old with the same level might face significant challenges. Clinicians often pair AMH testing with transvaginal ultrasounds to count antral follicles, providing a more comprehensive assessment. If your AMH falls below 0.8 ng/mL, fertility specialists may recommend aggressive stimulation protocols or suggest prioritizing immediate egg freezing over delaying the process.
For those with borderline or low AMH levels, proactive steps can optimize egg freezing outcomes. Start by consulting a reproductive endocrinologist to discuss tailored stimulation protocols, such as higher doses of follicle-stimulating hormone (FSH) or the addition of luteinizing hormone (LH) to improve ovarian response. Lifestyle adjustments—reducing alcohol intake, quitting smoking, and maintaining a healthy BMI—can also support ovarian function. While AMH is not modifiable, addressing controllable factors ensures the best possible results within your biological constraints.
A common misconception is that low AMH automatically disqualifies someone from successful egg freezing. While lower levels correlate with reduced egg quantity and quality, they do not eliminate the possibility of retrieval. Advances in fertility technology, such as individualized medication dosing and improved vitrification techniques, have enhanced outcomes for women with diminished ovarian reserve. For example, a 38-year-old with an AMH of 0.7 ng/mL might retrieve 4–6 mature eggs, sufficient for potential future use. The key is early intervention and realistic expectations.
Ultimately, AMH testing is not a definitive verdict but a tool for informed decision-making. If your AMH is low, view it as a call to action rather than a barrier. Discuss all available options with your fertility specialist, including the potential for multiple retrieval cycles or donor eggs if necessary. Egg freezing remains a viable option for many, even with suboptimal AMH levels, provided the process is approached strategically and promptly. Knowledge of your ovarian reserve empowers you to take control of your fertility journey, ensuring the best chance of success.
Does PwC Cover Egg Freezing Costs? Benefits Explained
You may want to see also
Explore related products





![]()
Impact of Age on AMH Levels
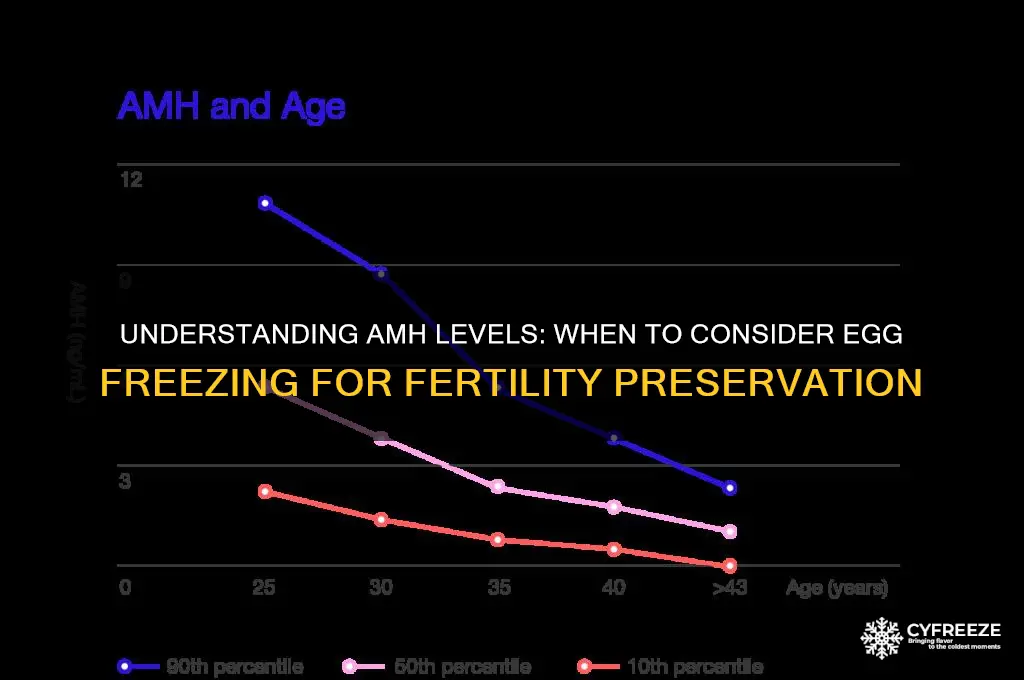
Anti-Müllerian hormone (AMH) levels serve as a critical marker of ovarian reserve, reflecting the number of remaining eggs. As women age, AMH levels naturally decline, mirroring the diminishing quantity and quality of ovarian follicles. By age 25, the average AMH level is around 4.0 ng/mL, but this drops to approximately 1.0 ng/mL by age 35 and often falls below 0.5 ng/mL by age 40. This decline accelerates after age 35, making it a pivotal factor in fertility decisions, particularly for those considering egg freezing.
For women contemplating egg freezing, understanding the threshold of AMH levels is essential. Clinics often consider AMH levels below 1.0 ng/mL as a red flag, indicating a lower ovarian reserve and potentially fewer eggs retrieved during the freezing process. However, even with levels as low as 0.5 ng/mL, egg freezing can still be successful, though the yield may be lower. Women with AMH levels below 0.3 ng/mL may face significant challenges, as the ovarian response to stimulation medications is often poor, requiring higher dosages of follicle-stimulating hormone (FSH) and a more tailored approach.
Age not only influences AMH levels but also the quality of the eggs retrieved. While a 30-year-old with an AMH of 2.0 ng/mL may have a higher success rate post-thaw, a 40-year-old with the same AMH level might face higher risks of chromosomal abnormalities. This underscores the importance of combining AMH levels with age-specific considerations when planning egg freezing. For instance, women over 38 may need to consider multiple cycles to ensure an adequate number of viable eggs, even if their AMH levels are relatively stable.
Practical steps for women with low AMH levels include consulting a reproductive endocrinologist early, as individualized protocols can optimize outcomes. Medications like DHEA (dehydroepiandrosterone) at 75 mg daily have shown promise in improving ovarian response in some cases, though results vary. Additionally, adopting a fertility-friendly lifestyle—such as maintaining a healthy weight, reducing stress, and avoiding smoking—can support ovarian function. While age and AMH levels are non-negotiable, proactive measures can maximize the chances of a successful egg freezing experience.
Eva Longoria's Fertility Journey: Did She Freeze Her Eggs?
You may want to see also
Frequently asked questions
AMH (Anti-Müllerian Hormone) is a hormone produced by ovarian follicles and is used as a marker of ovarian reserve. Lower AMH levels may indicate a reduced egg count, which can impact the success of egg freezing.
There’s no strict cutoff, but AMH levels below 1.0 ng/ml are generally considered low. If your AMH is in this range or declining rapidly, fertility specialists may recommend freezing eggs sooner rather than later.
Yes, egg freezing is still possible with low AMH, but the number of eggs retrieved may be lower. Your doctor may recommend additional stimulation protocols to maximize the yield.
Not necessarily. Success depends on factors like egg quality, age, and overall health. While low AMH may reduce the number of eggs retrieved, some women with low AMH still achieve successful pregnancies with frozen eggs.
If your AMH is borderline low (e.g., 1.0–1.5 ng/ml), it’s a good idea to consult a fertility specialist. They can assess your individual situation and advise whether egg freezing is a prudent step to preserve fertility.