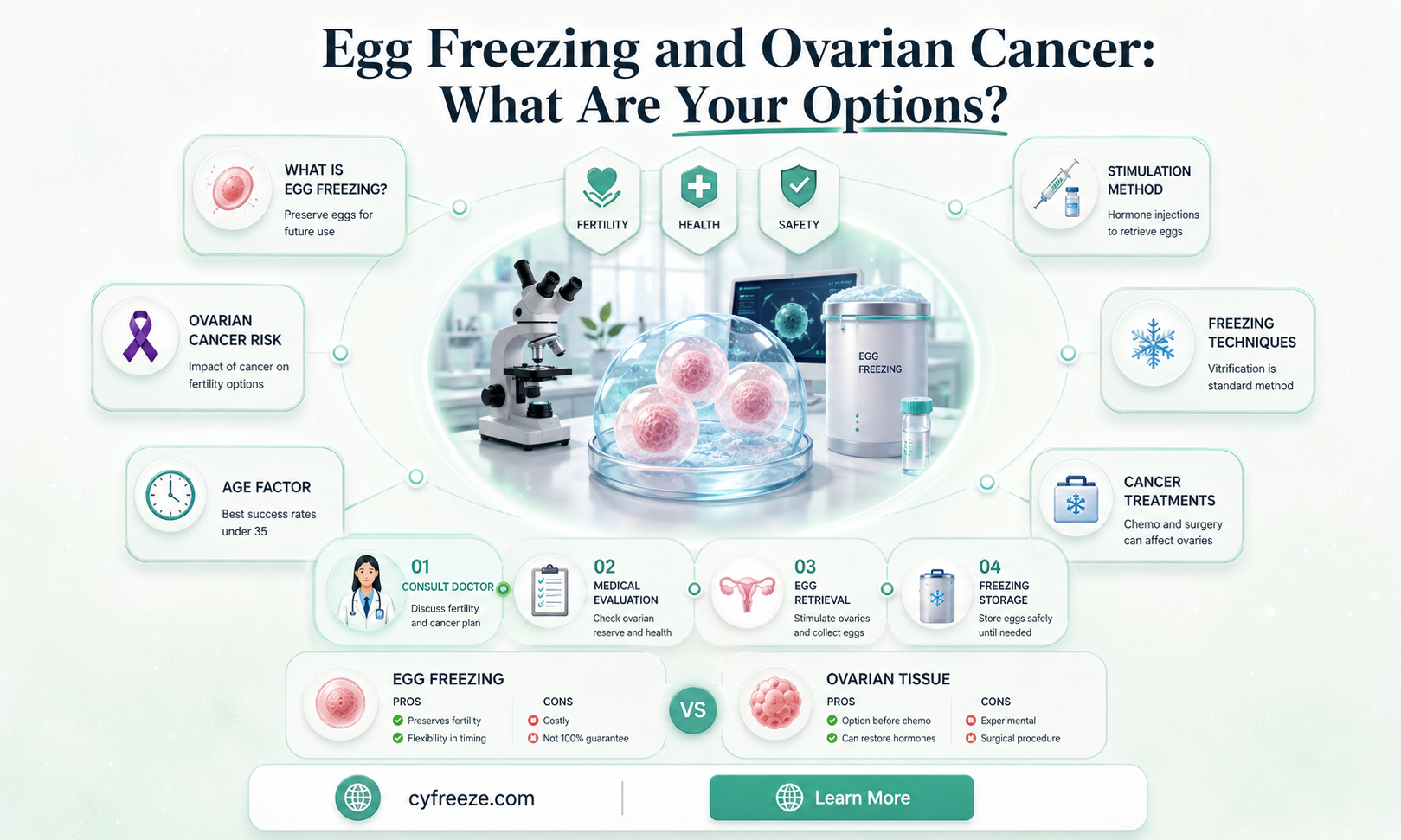
When considering fertility preservation options, individuals diagnosed with ovarian cancer often face complex decisions, including whether they can freeze their eggs. Ovarian cancer and its treatments, such as surgery, chemotherapy, or radiation, can significantly impact ovarian function and fertility. While egg freezing (oocyte cryopreservation) is a viable option for many, its feasibility for those with ovarian cancer depends on several factors, including the stage of cancer, the urgency of treatment, and the individual’s overall health. In some cases, egg freezing may be possible before treatment begins, but it requires careful coordination with oncologists and fertility specialists to ensure safety and effectiveness. However, if the cancer is advanced or if treatment is immediate, other fertility preservation methods or alternatives may need to be explored. Consulting with a multidisciplinary team is essential to weigh the risks, benefits, and timing of egg freezing in the context of ovarian cancer.
| Characteristics | Values |
|---|---|
| Eligibility | Generally possible, but depends on individual case and cancer stage. Consultation with oncologist and fertility specialist is essential. |
| Timing | Ideally before cancer treatment starts, as chemotherapy and radiation can damage eggs. |
| Procedure | Similar to standard egg freezing (oocyte cryopreservation): ovarian stimulation, egg retrieval, and freezing. |
| Success Rates | Varies; may be lower due to potential ovarian damage from cancer or prior treatments. |
| Risks | Ovarian stimulation may temporarily increase estrogen levels, which could be a concern for hormone-sensitive cancers. Procedure-related risks (e.g., infection, bleeding) are minimal. |
| Cost | Typically $10,000–$15,000 per cycle, plus annual storage fees ($500–$1,000). Insurance coverage varies. |
| Alternatives | Embryo freezing (if partnered), ovarian tissue cryopreservation (experimental for cancer patients). |
| Emotional Impact | Can provide hope for future fertility but may add stress during cancer treatment. |
| Long-term Outcomes | Limited data, but frozen eggs can lead to successful pregnancies post-cancer treatment. |
| Medical Advancements | Ongoing research to improve safety and efficacy for cancer patients. |
Explore related products





What You'll Learn
![]()
Eligibility for egg freezing with ovarian cancer diagnosis
An ovarian cancer diagnosis raises immediate concerns about fertility preservation, and egg freezing is often a critical consideration. Eligibility for this procedure hinges on several factors, including the stage of cancer, overall health, and the urgency of treatment. Early-stage ovarian cancer patients may have a window of opportunity to undergo egg freezing before starting chemotherapy or surgery, which can compromise ovarian function. However, advanced stages often require immediate intervention, leaving little time for fertility preservation. Consulting with an oncologist and reproductive specialist is essential to assess individual circumstances and determine feasibility.
The process of egg freezing involves ovarian stimulation, where medications like gonadotropins are administered to encourage the development of multiple follicles. For ovarian cancer patients, this step requires careful monitoring to avoid exacerbating the condition. Protocols may be adjusted to minimize hormonal stimulation, particularly in cases where estrogen-sensitive tumors are present. Typically, stimulation lasts 8–14 days, followed by a trigger shot (e.g., hCG or GnRH agonist) to finalize egg maturation before retrieval. Timing is critical, as delays can interfere with cancer treatment schedules.
Age plays a significant role in eligibility, as ovarian reserve declines with age, reducing the likelihood of successful egg retrieval. Women under 35 generally have higher success rates, but those in their late 30s or early 40s may still be candidates, depending on their ovarian reserve. Tests like AMH (anti-Müllerian hormone) levels and antral follicle counts can provide insights into fertility potential. For ovarian cancer patients, these assessments must be weighed against the urgency of cancer treatment, as delaying therapy can pose serious risks.
Practical considerations include the emotional and financial burden of egg freezing. The procedure can cost between $10,000 and $15,000 per cycle, with additional annual storage fees of $300–$500. Insurance coverage varies, and ovarian cancer patients may face limited options due to their diagnosis. Support from fertility preservation programs or financial assistance initiatives can help alleviate some of these challenges. Additionally, patients should be prepared for the emotional toll of balancing cancer treatment with fertility decisions, often requiring counseling or support groups.
Ultimately, eligibility for egg freezing with an ovarian cancer diagnosis is a complex, individualized decision. While it offers hope for future fertility, it must be carefully balanced against the immediate need for cancer treatment. Patients should work closely with a multidisciplinary team to explore all options, including alternative methods like embryo freezing or ovarian tissue cryopreservation. Early consultation and proactive planning are key to maximizing the chances of preserving fertility while prioritizing health and safety.
Egg Freezing Costs in California: What to Expect Financially
You may want to see also
Explore related products






![]()
Timing of egg retrieval before cancer treatment
For women diagnosed with ovarian cancer, the urgency to preserve fertility often collides with the immediate need for cancer treatment. Egg retrieval, a critical step in fertility preservation, must be timed meticulously to balance the race against cancer progression with the biological realities of ovarian stimulation. The window for intervention is narrow, typically ranging from 10 to 14 days, depending on the stimulation protocol. Standard ovarian stimulation protocols, which involve medications like gonadotropins (e.g., follicle-stimulating hormone, or FSH) to mature multiple eggs, usually take 8–12 days. However, in the context of ovarian cancer, this process must be expedited without compromising the patient’s safety or treatment timeline.
Accelerated protocols, often referred to as "random start" or "antagonist protocols," have been developed to shorten the stimulation phase to as little as 5–7 days. These protocols bypass the need to synchronize with the menstrual cycle, allowing for immediate initiation of stimulation regardless of the patient’s cycle phase. For example, a patient might begin with a daily dose of 150–225 IU of FSH, combined with a gonadotropin-releasing hormone (GnRH) antagonist like cetrorelix or ganirelix to prevent premature ovulation. This approach minimizes delays but requires careful monitoring via transvaginal ultrasound and hormone level checks to ensure follicular development without exacerbating the cancer.
The timing of egg retrieval is further complicated by the need to avoid delaying cancer treatment, which can worsen prognosis. Studies suggest that a delay of 2–4 weeks for fertility preservation is generally acceptable for early-stage ovarian cancer but may be riskier in advanced cases. In such scenarios, a "rescue" approach—where eggs are retrieved without full stimulation—may be considered, though success rates are lower. For instance, if a patient’s cancer is aggressive and requires immediate surgery, immature eggs can be extracted during the procedure and matured in vitro, though this technique is still experimental and not widely available.
Practical considerations also play a role. Patients must be informed that fertility preservation may not always be feasible, especially if cancer has spread extensively or if the patient is critically ill. Additionally, the emotional toll of making rapid decisions about fertility while processing a cancer diagnosis cannot be understated. Support from a multidisciplinary team, including oncologists, reproductive endocrinologists, and mental health professionals, is essential to navigate these complexities.
In conclusion, the timing of egg retrieval before ovarian cancer treatment is a delicate balance of medical urgency, biological constraints, and patient priorities. While accelerated protocols offer a viable option, they require precise coordination and individualized care. Patients and providers must weigh the risks and benefits, ensuring that every effort is made to preserve fertility without compromising cancer treatment outcomes.
Freezing Curried Egg Sandwiches: Tips for Preserving Flavor and Texture
You may want to see also
Explore related products






![]()
Risks of ovarian stimulation during cancer
Ovarian stimulation, a critical step in egg freezing, involves administering hormones to stimulate the ovaries to produce multiple mature eggs. For women with ovarian cancer, this process introduces unique risks that must be carefully considered. The primary concern is the potential for hormone-based stimulation to exacerbate cancer growth, particularly in hormone-sensitive tumors. Ovarian cancers, especially those driven by estrogen or other hormones, may respond adversely to the elevated hormone levels induced by medications like follicle-stimulating hormone (FSH) or luteinizing hormone (LH). Studies suggest that estrogen, a key hormone in ovarian stimulation protocols, could theoretically promote the proliferation of cancer cells, though definitive evidence remains limited.
From a procedural standpoint, ovarian stimulation typically involves daily injections of gonadotropins, such as recombinant FSH, at doses ranging from 150 to 300 IU per day, depending on individual response. For cancer patients, this regimen poses a dilemma: while lower doses might reduce hormone exposure, they may also compromise egg yield, limiting the chances of successful fertility preservation. Additionally, the process requires frequent transvaginal ultrasounds and blood tests to monitor follicle development, which can be physically and emotionally taxing for someone already navigating a cancer diagnosis. These logistical challenges underscore the need for a tailored approach that balances fertility goals with oncological safety.
A comparative analysis of risks versus benefits is essential in this context. For younger patients, particularly those under 35 with early-stage ovarian cancer, the urgency to preserve fertility may outweigh the theoretical risks of stimulation. However, for older patients or those with advanced or hormone-sensitive cancers, the potential harm may outweigh the benefits. For instance, clear cell and endometrioid ovarian cancers are more likely to be hormone-sensitive, making stimulation riskier in these cases. Conversely, mucinous or low-grade serous cancers are less likely to be influenced by hormonal changes, offering a slightly safer window for intervention.
Practical tips for minimizing risks include opting for a "random start" protocol, which bypasses the need for hormone suppression and reduces overall hormone exposure. Another strategy is to use letrozole, an aromatase inhibitor, alongside stimulation medications to mitigate estrogen levels. However, these approaches are not universally applicable and require careful consultation with both oncologists and reproductive endocrinologists. Ultimately, the decision to proceed with ovarian stimulation must be made on a case-by-case basis, factoring in cancer type, stage, and individual health status. For some, alternative methods like ovarian tissue cryopreservation may be a safer, albeit less established, option.
Freeze Eggs for Meal Prep: A Time-Saving Kitchen Hack
You may want to see also
Explore related products





![]()
Success rates of egg freezing post-cancer treatment
Egg freezing after ovarian cancer treatment is a complex but increasingly viable option for preserving fertility. Success rates hinge on several factors, including the patient’s age at the time of freezing, the stage and aggressiveness of the cancer, and the timing of the procedure relative to treatment. Younger patients, typically under 35, tend to have higher success rates due to better egg quality. For instance, studies show that women under 35 may achieve live birth rates of up to 40-50% per thawed egg, compared to 20-30% for those over 38. However, ovarian cancer survivors face unique challenges, such as potential damage to ovarian reserve from chemotherapy or surgery, which can reduce the number of viable eggs retrieved.
The process of egg freezing post-cancer treatment requires careful coordination between oncologists and reproductive specialists. Ideally, egg retrieval should occur before cancer treatment begins, but this isn’t always possible. If freezing happens after treatment, patients must wait until they are in remission, typically 2-5 years, to ensure cancer-free status. During this period, ovarian stimulation protocols may need adjustment, as standard dosages of medications like gonadotropins (e.g., 150-300 IU daily) might be less effective in cancer survivors. Monitoring follicle development through frequent ultrasounds and hormone level checks is critical to optimizing outcomes.
Comparatively, success rates for ovarian cancer survivors are lower than those for women freezing eggs for non-medical reasons. A 2021 study found that only 15-25% of thawed eggs from cancer survivors resulted in live births, partly due to compromised ovarian function post-treatment. However, advancements in vitrification (a rapid freezing technique) have improved egg survival rates to over 90%, offering hope. Additionally, using donor eggs or embryos can significantly increase success rates, though this decision depends on individual circumstances and preferences.
Practical tips for maximizing success include maintaining a healthy lifestyle post-treatment, as factors like BMI and smoking can impact fertility. Patients should also inquire about fertility preservation options at diagnosis, even if immediate freezing isn’t feasible. Financial planning is crucial, as egg freezing and storage can cost $10,000-$15,000 initially, with annual storage fees of $500-$1,000. Some insurance plans or cancer support organizations may offer assistance, making it essential to explore all resources.
In conclusion, while success rates for egg freezing post-ovarian cancer treatment are lower than average, they remain a valuable option for many. With careful planning, personalized medical protocols, and realistic expectations, survivors can increase their chances of achieving pregnancy. Consulting a fertility specialist early in the cancer journey is key to navigating this complex but potentially life-changing process.
Can You Freeze Eggs? A Guide to Preserving Freshness and Quality
You may want to see also
Explore related products





![]()
Alternative fertility preservation options for cancer patients
For ovarian cancer patients, egg freezing may not always be feasible due to the urgency of treatment or the cancer's impact on ovarian function. However, alternative fertility preservation options exist, offering hope for future family planning. One such method is embryo cryopreservation, where eggs are fertilized with sperm before freezing, creating embryos for later use. This approach requires a partner or donor sperm and is often recommended for patients with time before treatment begins. Success rates vary but can be higher than egg freezing alone, particularly for women over 35.
Another option is oocyte maturation in vitro, a technique where immature eggs are retrieved and matured in a lab before freezing. This method is beneficial for patients who cannot undergo hormone stimulation due to estrogen-sensitive cancers. While still experimental, it has shown promise in preserving fertility without delaying cancer treatment. Patients should consult their oncologist and reproductive specialist to weigh the risks and benefits, as the procedure’s effectiveness depends on individual health factors.
For those with advanced ovarian cancer or compromised ovarian function, ovarian tissue cryopreservation may be considered. This involves removing and freezing a portion of the ovary, which can later be reimplanted to restore fertility. Though less common, it has resulted in live births and is particularly useful for prepubescent girls or women who cannot delay treatment. However, the risk of reintroducing cancer cells must be carefully evaluated, especially in ovarian cancer cases.
Finally, adoption and surrogacy remain viable alternatives for cancer survivors who cannot pursue biological parenthood. While not medical procedures, these options provide pathways to building a family post-treatment. Financial and emotional considerations are significant, but support from fertility counselors and advocacy groups can help navigate these choices. Each alternative requires careful planning and consultation with medical professionals to align with the patient’s health and goals.
Freezing Scrambled Eggs for Baby: A Safe and Convenient Option?
You may want to see also
Frequently asked questions
Yes, egg freezing (oocyte cryopreservation) is possible for some women with ovarian cancer, but it depends on the stage of cancer, treatment plan, and individual health status. Consult with your oncologist and fertility specialist to assess your options.
Egg freezing before treatment is generally safe if done before chemotherapy or radiation begins. However, the process must be timed carefully to avoid delaying cancer treatment, as some therapies can harm fertility.
Yes, treatments like chemotherapy or radiation can reduce ovarian reserve and impact egg quality. Egg freezing is most effective if done before cancer treatment starts, as it may not be possible or successful afterward.
The primary risk is the hormonal stimulation required for egg retrieval, which may not be suitable for all cancer patients. Additionally, delaying cancer treatment for egg freezing can be risky, so careful coordination is essential.
Yes, if the egg freezing process was successful, the eggs can be used for in vitro fertilization (IVF) after cancer treatment and recovery, provided your health allows it. Discuss long-term fertility plans with your healthcare team.



















