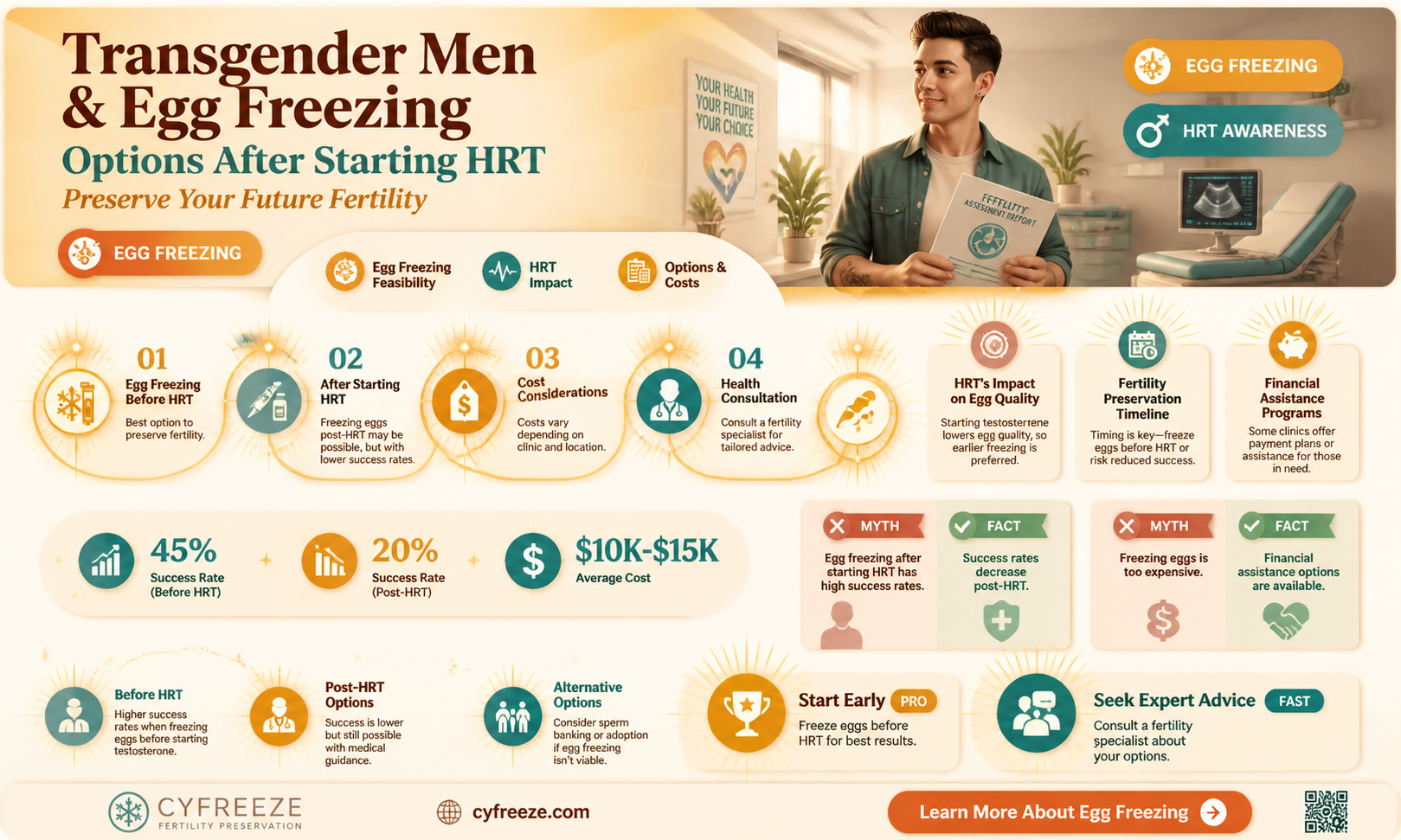
Transgender men who have started hormone replacement therapy (HRT) often face unique considerations when it comes to fertility preservation, including the possibility of freezing their eggs. While HRT, particularly testosterone, can suppress ovarian function and reduce fertility over time, it does not immediately eliminate the potential for egg retrieval. However, the success of egg freezing for transgender men on HRT depends on various factors, such as the duration of testosterone use, individual ovarian response, and overall health. Consulting with a reproductive endocrinologist or fertility specialist is crucial to assess viability, discuss potential risks, and explore options for preserving fertility before or during HRT. Early planning and open communication with healthcare providers are key to making informed decisions about this important aspect of family planning.
| Characteristics | Values |
|---|---|
| Possibility of Egg Freezing | Yes, transgender men can freeze their eggs after starting HRT. |
| Effect of Testosterone on Ovarian Reserve | Testosterone may reduce ovarian reserve over time, making egg retrieval more challenging. |
| Timing Recommendation | Ideally, egg freezing should be considered before starting HRT or early in HRT for better outcomes. |
| Success Rates | Success rates vary but are generally lower compared to those who freeze eggs before HRT. |
| Medical Evaluation | Requires consultation with a fertility specialist to assess ovarian reserve and suitability. |
| Procedure | Involves ovarian stimulation, egg retrieval, and cryopreservation. |
| Cost | Expensive; costs vary by location and clinic, typically ranging from $10,000 to $15,000. |
| Emotional Considerations | May involve emotional and identity-related decisions regarding fertility preservation. |
| Legal and Ethical Aspects | Legal and ethical considerations vary by region; some areas may have restrictions. |
| Alternative Options | Embryo freezing or donor eggs may be considered if egg freezing is not feasible. |
Explore related products





What You'll Learn
![]()
Eligibility for egg freezing post-HRT
Transgender men considering egg freezing after starting hormone replacement therapy (HRT) face unique eligibility criteria shaped by medical, hormonal, and reproductive factors. While HRT is essential for gender affirmation, its impact on ovarian function complicates the feasibility of egg retrieval. Testosterone, the primary hormone in masculinizing HRT, suppresses ovulation and reduces ovarian reserve over time, making timely intervention critical. Most fertility specialists recommend freezing eggs before initiating HRT or within the first 6–12 months of treatment, as prolonged exposure to testosterone may diminish egg quality and quantity.
Steps to Assess Eligibility Post-HRT
If HRT has already begun, eligibility for egg freezing hinges on individualized assessment. A baseline ovarian reserve test, such as an antral follicle count (AFC) or anti-Müllerian hormone (AMH) level, is essential. AMH values below 1.0 ng/mL or an AFC under 5–7 follicles per ovary may indicate reduced fertility potential. However, some individuals with lower reserves still produce viable eggs, so consultation with a reproductive endocrinologist is crucial. Additionally, a temporary pause in testosterone (under medical supervision) may be advised to stimulate ovarian activity, though this decision must balance fertility goals with mental health and gender affirmation needs.
Cautions and Considerations
Egg freezing post-HRT is not without risks. Ovarian stimulation protocols, which use medications like gonadotropins to induce multiple follicle growth, may be less effective in individuals on testosterone. Higher doses or extended stimulation cycles might be required, increasing the risk of ovarian hyperstimulation syndrome (OHSS). Psychological considerations are equally important; halting or reducing testosterone, even temporarily, can trigger dysphoria or emotional distress. Clinicians must collaborate with patients to develop a plan that respects their gender identity while maximizing fertility preservation chances.
Practical Tips for Success
For transgender men exploring this option, early action is paramount. Documenting ovarian reserve before starting HRT provides a benchmark for future decisions. If HRT is already underway, monitor ovarian response closely through regular AMH testing and ultrasounds. Consider clinics experienced in LGBTQ+ fertility care, as they are more likely to provide culturally competent guidance. Finally, explore financial assistance or insurance coverage, as egg freezing can cost $10,000–$15,000 per cycle, with additional annual storage fees of $300–$500.
Master the Art of Freezing Eggs: A Simple, Effective Guide
You may want to see also
Explore related products






![]()
Impact of testosterone on ovarian function
Testosterone therapy, a cornerstone of gender-affirming treatment for transgender men, significantly impacts ovarian function, raising critical considerations for those exploring fertility preservation options like egg freezing. The ovaries, sensitive to hormonal fluctuations, respond to testosterone by downregulating their typical estrogen-driven processes. Studies indicate that even low to moderate doses of testosterone (50-100 mg weekly) can suppress follicle-stimulating hormone (FSH) and luteinizing hormone (LH), key players in ovulation. This suppression often leads to amenorrhea (absence of menstruation) within 3-6 months of starting HRT, signaling a decline in ovarian activity. For transgender men contemplating egg freezing, this timeline underscores the urgency of acting before initiating testosterone, as ovarian reserve diminishes once HRT begins.
From a comparative standpoint, the impact of testosterone on ovarian function mirrors, yet contrasts with, the effects of natural aging. While aging gradually reduces ovarian reserve due to follicle depletion, testosterone accelerates this process by disrupting the hormonal feedback loop essential for ovulation. A 2021 study published in *Human Reproduction* found that transgender men on testosterone for over 12 months exhibited significantly lower anti-Müllerian hormone (AMH) levels—a marker of ovarian reserve—compared to cisgender women of the same age. This suggests that testosterone not only pauses ovarian function but may also irreversibly reduce the number of viable eggs available for retrieval. For those in their late 20s to early 30s, a common age range for transgender men starting HRT, this highlights the narrow window for successful egg freezing.
Persuasively, the evidence points to a clear takeaway: delaying testosterone therapy until after egg freezing is the most effective strategy for preserving fertility. However, this decision is deeply personal, balancing the desire for gender-affirming care with future family planning. For those already on testosterone, the situation is more complex. Some clinicians recommend a temporary pause in HRT (3-4 weeks) to stimulate ovarian function before egg retrieval, though success rates vary. A 2020 case series in *Fertility and Sterility* reported successful egg retrieval in 60% of transgender men who temporarily discontinued testosterone, but this approach requires careful monitoring to avoid psychological distress from estrogen rebound.
Practically, transgender men considering egg freezing should consult a reproductive endocrinologist before starting HRT. Key steps include baseline AMH testing, transvaginal ultrasound to assess ovarian reserve, and a detailed discussion of expectations. For those already on testosterone, a tailored protocol may involve gonadotropin stimulation during the HRT pause, with retrieval ideally performed within 6-12 months of starting testosterone to maximize yield. Costs, ranging from $7,000 to $15,000 per cycle, and emotional considerations should also be factored into decision-making. Ultimately, while testosterone’s impact on ovarian function poses challenges, proactive planning and medical collaboration can help navigate this intersection of gender affirmation and fertility preservation.
Freezing Eggs Whole: A Complete Guide to Preserving Freshness
You may want to see also
Explore related products






![]()
Success rates of egg retrieval
Transgender men considering egg retrieval and freezing after starting hormone replacement therapy (HRT) often face uncertainty about success rates. Research indicates that while HRT can suppress ovarian function, it does not permanently eliminate the possibility of egg retrieval. Success rates vary based on factors such as the duration of HRT, the individual’s age, and the specific hormones used. For instance, testosterone, commonly used in HRT for transgender men, can reduce ovarian reserve over time but does not immediately render egg retrieval impossible. Studies show that individuals who undergo egg retrieval within the first 2–3 years of HRT tend to have higher success rates compared to those who wait longer.
Analyzing success rates requires understanding the ovarian response to stimulation protocols. Typically, transgender men undergo controlled ovarian stimulation (COS) using medications like gonadotropins to induce follicle growth. The average number of eggs retrieved ranges from 5 to 15 per cycle, though this can vary widely. Younger individuals (under 30) generally achieve higher retrieval numbers due to greater ovarian reserve. For example, a 25-year-old transgender man who has been on testosterone for 1 year might retrieve 10–12 eggs, while a 35-year-old with 5 years of HRT may retrieve 3–5 eggs. These numbers are influenced by individual biology and the cumulative effects of testosterone on ovarian function.
Practical steps to optimize success include consulting a reproductive endocrinologist early in the transition process. Temporarily pausing testosterone for 3–6 months before egg retrieval can improve ovarian response, though this decision should be weighed against personal gender affirmation goals. Additionally, using lower testosterone doses (e.g., 50–100 mg every 2 weeks instead of 100–200 mg) may slow ovarian suppression while maintaining masculinizing effects. Monitoring ovarian reserve through blood tests (e.g., anti-Müllerian hormone, or AMH) and ultrasounds can provide insights into the timing and feasibility of egg retrieval.
Comparatively, success rates for transgender men are often lower than those for cisgender women undergoing fertility preservation due to the added variable of HRT. However, advancements in reproductive technology, such as improved stimulation protocols and vitrification (a rapid freezing technique), have enhanced outcomes. For instance, vitrification achieves egg survival rates of over 90%, with fertilization rates comparable to fresh eggs. While not every retrieved egg will result in a viable embryo, freezing multiple eggs increases the chances of future successful pregnancies.
In conclusion, while HRT complicates egg retrieval for transgender men, success is achievable with careful planning and medical guidance. Early intervention, personalized hormone management, and collaboration with fertility specialists are key to maximizing retrieval rates. Transgender men should approach this process with realistic expectations, understanding that individual outcomes vary but that many have successfully preserved their fertility post-HRT.
Freezing Egg Roll Wrappers: A Handy Storage Solution for Freshness
You may want to see also
Explore related products





![]()
Risks and complications of the procedure
Transgender men considering egg freezing after starting hormone replacement therapy (HRT) face unique risks and complications tied to both their hormonal state and the procedure itself. Testosterone, a cornerstone of masculinizing HRT, suppresses ovarian function, reducing the number of eggs retrieved during the freezing process. This hormonal interference necessitates higher doses of ovarian stimulation medications, such as gonadotropins, to induce follicle growth. For instance, a typical stimulation protocol might involve daily injections of 150–300 IU of follicle-stimulating hormone (FSH) for 8–14 days, compared to lower doses used in cisgender women. This intensified regimen increases the risk of ovarian hyperstimulation syndrome (OHSS), a potentially severe condition marked by fluid accumulation in the abdomen and chest, which occurs in up to 10% of egg freezing cycles.
Another critical concern is the impact of long-term testosterone use on egg quality. While research is limited, studies suggest that prolonged exposure to testosterone may alter ovarian reserve and egg viability. A 2021 study published in the *Journal of Assisted Reproduction and Genetics* found that transgender men on HRT had lower antral follicle counts, a key predictor of ovarian reserve, compared to cisgender women. This reduction in egg quantity and quality could diminish the success rates of future fertility treatments, such as in vitro fertilization (IVF), even with frozen eggs. Prospective parents should weigh these risks against their desire to preserve fertility, ideally consulting a reproductive endocrinologist before initiating HRT.
The timing of egg freezing relative to HRT initiation also plays a pivotal role in mitigating risks. Transgender men who freeze their eggs before starting testosterone or within the first six months of HRT generally achieve better outcomes. After this window, ovarian suppression becomes more pronounced, complicating the stimulation process. For example, a 2020 study in *Human Reproduction* reported that transgender men who underwent egg freezing within one year of starting HRT had a 30% higher retrieval rate compared to those who waited longer. Practical advice includes pausing testosterone temporarily during the egg freezing cycle, though this decision must balance fertility goals with gender-affirming care, under medical supervision.
Psychological and emotional complications cannot be overlooked. The egg freezing process involves daily injections, frequent monitoring, and invasive procedures, which can be physically and emotionally taxing. For transgender men, this experience may conflict with their gender identity, particularly if the process requires temporary testosterone cessation. A 2019 survey in *LGBTQ+ Health* highlighted that 40% of transgender men reported distress related to fertility preservation procedures. Support from mental health professionals and LGBTQ+-affirming healthcare teams is essential to navigate these challenges.
Finally, financial and logistical barriers compound the risks. Egg freezing is costly, typically ranging from $10,000 to $15,000 per cycle, excluding medication and storage fees. Insurance coverage for transgender individuals varies widely, often leaving patients to bear the expense. Additionally, not all fertility clinics are equipped to address the unique needs of transgender men, necessitating careful provider selection. Practical tips include researching clinics with experience in transgender care, exploring financial assistance programs, and discussing all potential risks with a healthcare team before proceeding. While egg freezing offers a pathway to parenthood, its risks and complications demand careful consideration and individualized planning.
Egg Freezing and Infertility: Debunking Myths and Understanding Risks
You may want to see also
Explore related products





![]()
Legal and ethical considerations for trans men
Transgender men seeking to preserve fertility through egg freezing after starting hormone replacement therapy (HRT) face a complex web of legal and ethical considerations. One critical issue is the variability in legal recognition of transgender identities across jurisdictions. In countries or states where gender transition is not legally acknowledged, trans men might encounter barriers to accessing fertility preservation services. For instance, some clinics require legal documentation matching the individual’s gender identity, which can exclude those whose identification documents have not been updated. This discrepancy highlights the need for standardized policies that prioritize medical necessity over bureaucratic hurdles, ensuring equitable access to reproductive care.
Ethically, informed consent emerges as a cornerstone in this process. Fertility clinics must provide trans men with comprehensive information about the potential risks and uncertainties of egg freezing post-HRT. Testosterone, a key component of HRT for trans men, can suppress ovarian function, potentially reducing the number of viable eggs retrieved. Clinicians should discuss these risks openly, alongside the emotional and financial implications of fertility preservation. For example, a 25-year-old trans man might be advised to consider egg freezing within the first year of HRT, as prolonged testosterone use could diminish ovarian reserve. Transparent communication ensures individuals make decisions aligned with their long-term goals.
Another ethical consideration is the intersection of reproductive rights and gender affirmation. Some argue that prioritizing fertility preservation could inadvertently pressure trans men to delay HRT, potentially compromising their mental health and well-being. This tension underscores the importance of framing fertility preservation as an option, not an obligation. Healthcare providers should emphasize that pursuing HRT and preserving fertility are not mutually exclusive, especially with advancements in reproductive technologies. For instance, protocols allowing for temporary HRT pauses or adjustments (e.g., reducing testosterone dosage to 50 mg weekly for a month) have shown promise in stimulating ovarian activity for egg retrieval.
Legally, the status of frozen eggs in the context of transgender identity raises questions about parental rights and inheritance. In jurisdictions where parentage laws are not inclusive of transgender individuals, trans men might face challenges in being recognized as legal parents of children conceived through their frozen eggs. Advocacy for updated legislation that reflects the diversity of family structures is essential. For example, countries like Canada and the Netherlands have enacted laws explicitly protecting the parental rights of transgender individuals, setting a precedent for global reform.
In conclusion, navigating the legal and ethical landscape of egg freezing for trans men requires a multifaceted approach. Policymakers, healthcare providers, and advocates must collaborate to dismantle barriers, ensure informed consent, and uphold reproductive autonomy. By addressing these considerations, society can move toward a more inclusive framework that respects the rights and needs of transgender individuals seeking to preserve their fertility.
Easy Freezing Tips for Delicious, Make-Ahead Egg Muffins
You may want to see also
Frequently asked questions
Yes, transgender men can freeze their eggs after starting HRT, but the process may be more complex. HRT can suppress ovarian function, so it’s best to consult a fertility specialist early to assess options and timing.
HRT, particularly testosterone, can reduce ovarian responsiveness over time, potentially lowering the success rate of egg freezing. Early consultation with a fertility specialist is recommended to maximize chances.
It’s advisable to consider egg freezing before starting HRT or as early as possible after beginning it. Delaying HRT temporarily may be an option to allow for egg retrieval, but this should be discussed with a healthcare provider.
The primary risk is reduced ovarian response due to HRT, which may limit the number of eggs retrieved. However, the procedure itself carries minimal risks, similar to those for cisgender women undergoing egg freezing.