The use of embryos without freezing is a topic of growing interest in the field of assisted reproductive technology (ART), as it offers potential advantages such as reduced costs, simplified procedures, and minimized risks associated with cryopreservation. Fresh embryo transfers, where embryos are transferred to the uterus immediately after fertilization without undergoing freezing, have been traditionally practiced and continue to be a viable option in certain scenarios. Advances in laboratory techniques and a better understanding of embryonic development have further supported the feasibility of using fresh embryos, particularly in cases where the uterine environment is optimal for implantation. However, the decision to use fresh embryos versus frozen ones depends on various factors, including patient-specific conditions, ovarian response, and the overall treatment plan. As research progresses, the role of fresh embryo transfers in improving pregnancy outcomes and accessibility to fertility treatments remains a critical area of exploration.
| Characteristics | Values |
|---|---|
| Fresh Embryo Transfer | Possible and commonly used in IVF cycles. |
| Viability | Fresh embryos can be transferred immediately after fertilization. |
| Success Rates | Comparable to frozen embryo transfers in many cases. |
| Time Frame | Typically transferred within 1-5 days after egg retrieval. |
| Cost | Generally lower than frozen embryo transfers due to fewer procedures. |
| Indications | Preferred in patients with normal ovarian response and embryo quality. |
| Risks | Slightly higher risk of ovarian hyperstimulation syndrome (OHSS). |
| Patient Suitability | Suitable for patients without complex medical conditions. |
| Technology | No cryopreservation required; uses standard IVF lab techniques. |
| Regulatory Considerations | Subject to the same ethical and legal guidelines as frozen embryos. |
| Storage Requirements | None, as embryos are not stored. |
| Cycle Synchronization | Requires precise timing between egg retrieval and transfer. |
| Patient Convenience | Less invasive and time-consuming compared to frozen cycles. |
| Clinical Outcomes | Similar pregnancy and live birth rates to frozen transfers in many studies. |
| Availability | Widely available in most fertility clinics globally. |
Explore related products






What You'll Learn
![]()
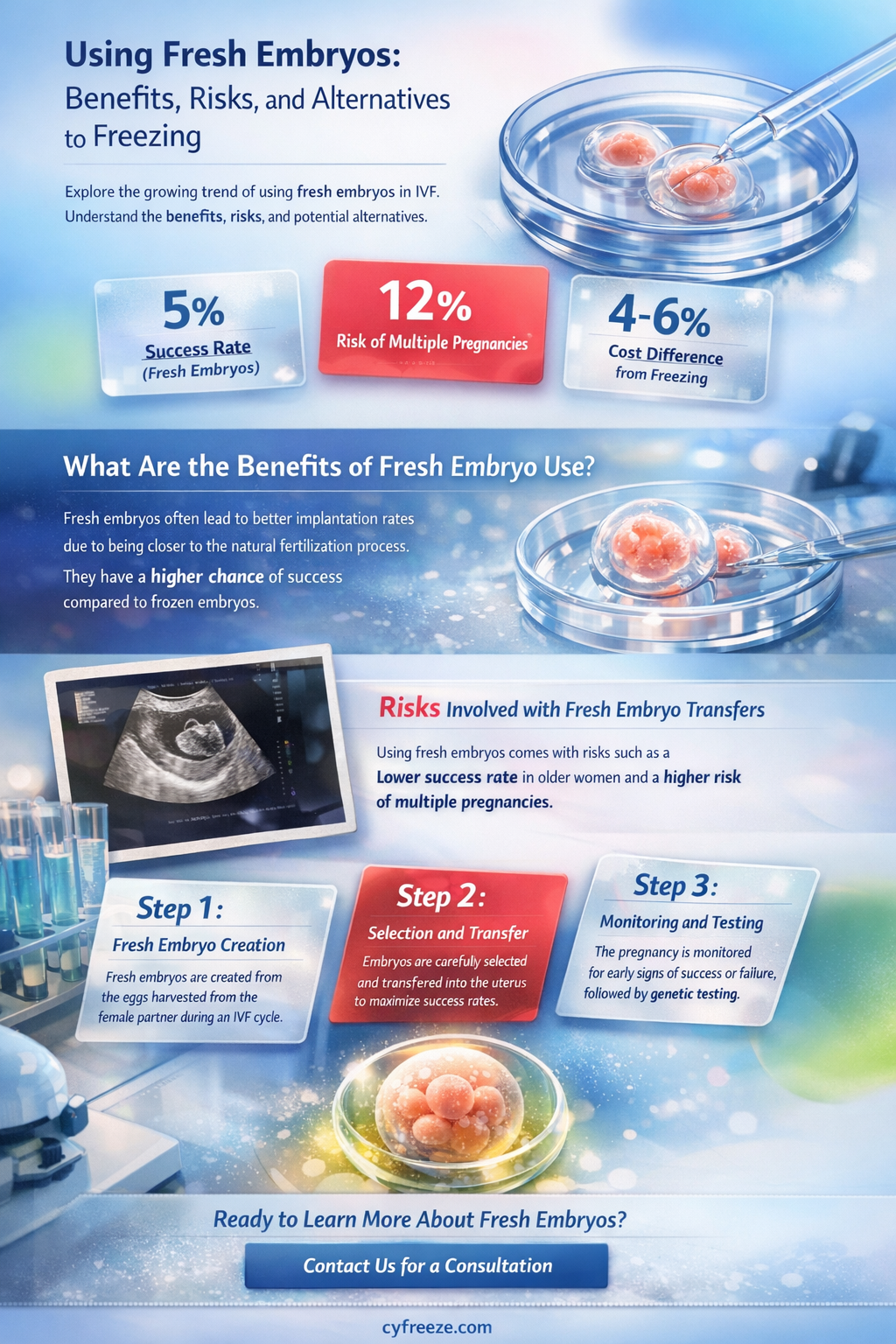
Fresh Embryo Transfer Benefits
Embryos can indeed be used without freezing, a process known as fresh embryo transfer (FET). This approach offers distinct advantages in assisted reproductive technology (ART), particularly for specific patient profiles and clinical scenarios. By bypassing the cryopreservation step, fresh transfers align more closely with the body’s natural reproductive timeline, potentially enhancing outcomes for certain individuals.
Analytical Perspective:
Fresh embryo transfers eliminate the risks associated with the freezing and thawing process, which can occasionally impact embryo viability. Studies indicate that fresh transfers may yield higher implantation rates in women under 35, particularly those with polycystic ovary syndrome (PCOS) or high ovarian reserve. For instance, a 2020 meta-analysis published in *Fertility and Sterility* found that fresh cycles resulted in a 38% live birth rate compared to 34% for frozen cycles in this demographic. The absence of cryopreservation also reduces costs and shortens treatment timelines, making it a practical choice for patients seeking immediate results.
Instructive Approach:
To optimize fresh embryo transfer success, clinicians typically follow a precise protocol. Ovarian stimulation is initiated with medications like gonadotropins (e.g., 150–300 IU daily) to encourage follicle development. Once follicles reach 18–20 mm, a trigger injection of human chorionic gonadotropin (hCG) or GnRH agonist is administered 36 hours before egg retrieval. Embryos are cultured for 1–3 days, then transferred using an ultrasound-guided catheter. Patients are advised to maintain a supine position for 15–30 minutes post-transfer and may be prescribed progesterone (200 mg vaginally or 1–2 mg intramuscularly daily) to support uterine lining receptivity.
Persuasive Argument:
Fresh embryo transfers are not just a relic of early ART practices but a strategic choice for modern fertility care. For patients with favorable prognoses, such as those with normal ovarian function and no history of implantation failure, fresh transfers offer a streamlined path to pregnancy. The psychological benefits are equally compelling: avoiding the wait associated with frozen cycles reduces anxiety and allows patients to proceed with treatment momentum. Additionally, fresh transfers are ideal for time-sensitive situations, such as when future fertility preservation is uncertain due to medical conditions like cancer.
Comparative Insight:
While frozen embryo transfers have gained popularity due to their flexibility and higher success rates in certain cases (e.g., patients with elevated progesterone or endometriosis), fresh transfers hold their ground in specific contexts. For example, fresh cycles are often preferred in low-resource settings where cryopreservation infrastructure is limited. Moreover, fresh transfers avoid the risk of embryo loss during the thawing process, which, though rare, can occur in 2–5% of cases. Clinicians must weigh these factors against individual patient needs, such as ovarian response and uterine environment, to determine the optimal approach.
Descriptive Takeaway:
Imagine a fertility journey where every step aligns with the body’s natural rhythm, from ovulation to implantation. Fresh embryo transfers embody this harmony, offering a direct route to parenthood for many. Picture a laboratory where embryos, nurtured for just a few days, are gently transferred into a receptive uterus, bypassing the icy pause of cryopreservation. This method, while not universally superior, shines as a beacon of hope for those whose biology and circumstances align with its strengths. It’s a reminder that in the intricate world of ART, sometimes the freshest approach is the most effective.
Portable Fat Freezing Machines: Effective At-Home Body Sculpting Solutions?
You may want to see also
Explore related products






![]()
Risks of Non-Frozen Embryo Use
Non-frozen embryo transfers, often referred to as fresh embryo transfers, are a common practice in assisted reproductive technologies (ART). While they offer certain advantages, such as avoiding the potential risks associated with the freezing and thawing process, they are not without their own set of challenges. One of the primary risks involves the increased likelihood of ovarian hyperstimulation syndrome (OHSS), a potentially severe condition that can occur following ovarian stimulation. OHSS is characterized by enlarged ovaries, abdominal pain, and in severe cases, fluid accumulation in the abdomen and chest, which can lead to respiratory distress. The risk of OHSS is particularly heightened in fresh cycles because the embryo transfer occurs in the same cycle as ovarian stimulation, when hormone levels are at their peak.
Another significant risk is the potential for reduced implantation rates compared to frozen embryo transfers. Studies have shown that the endometrial lining may not be optimally receptive during a fresh cycle due to the high levels of hormones, particularly estrogen and progesterone, which can disrupt the synchrony between the embryo and the endometrium. This asynchrony can lead to lower implantation rates and, consequently, lower pregnancy rates. For instance, a 2018 study published in *The New England Journal of Medicine* found that frozen embryo transfers resulted in higher live birth rates compared to fresh transfers in women with high ovarian response to stimulation.
Furthermore, fresh embryo transfers carry a higher risk of multiple pregnancies, particularly in cases where multiple embryos are transferred to increase the chances of implantation. Multiple pregnancies are associated with a range of complications, including preterm birth, low birth weight, and increased maternal risks such as preeclampsia and gestational diabetes. While the trend in ART has shifted towards single embryo transfers to mitigate these risks, the practice is not universally adopted, and multiple embryo transfers still occur, especially in fresh cycles where the outcome of a single transfer is less predictable.
From a practical standpoint, patients considering non-frozen embryo use should be aware of the specific risks and discuss them thoroughly with their healthcare provider. For example, women under 35 with a good ovarian reserve might be advised to consider freezing all embryos and opting for a frozen transfer in a subsequent cycle to reduce the risk of OHSS and improve implantation rates. Additionally, monitoring hormone levels closely during the stimulation phase can help identify patients at higher risk of OHSS, allowing for adjustments in the treatment protocol.
In conclusion, while non-frozen embryo transfers offer certain benefits, they come with distinct risks that require careful consideration. Patients and clinicians must weigh these risks against the potential advantages, taking into account individual health profiles and treatment goals. By doing so, they can make informed decisions that optimize the chances of a successful pregnancy while minimizing complications.
Chest Freezer Electricity Usage: How Much Power Does It Consume?
You may want to see also
Explore related products




![]()
Timing for Optimal Implantation
Embryo transfer timing is a critical factor in the success of fresh, non-frozen embryo implantation. The window for optimal implantation is narrow, typically occurring 1–5 days after ovulation, with the most receptive phase being 3–4 days post-ovulation. This period, known as the "window of implantation," aligns with the endometrial receptivity array (ERA), a molecular profile that ensures the uterus is primed for embryo attachment. For fresh embryo transfers, synchronizing this window with the embryo’s developmental stage is essential. For instance, a day-3 embryo transfer corresponds to the 3-day post-ovulation window, while a day-5 blastocyst transfer aligns with the 5-day window. Precision in timing increases implantation rates by up to 30%, according to studies in *Human Reproduction*.
To achieve this synchronization, clinicians rely on hormonal monitoring and ultrasound assessments. For women undergoing natural cycles, ovulation prediction kits and serial ultrasounds track follicle development, with the trigger shot (e.g., hCG 10,000 IU) administered when the lead follicle reaches 18–20 mm. Embryo transfer is then scheduled 72–120 hours post-trigger, depending on the embryo’s developmental stage. In medicated cycles, protocols like the luteal phase support with progesterone (200 mg/day vaginally) begin on the day of ovulation retrieval, ensuring the endometrium remains receptive. Deviations from this timing, such as transferring a blastocyst on day 3 or vice versa, can reduce implantation rates by 15–20%.
A comparative analysis of fresh vs. frozen embryo transfers reveals that fresh cycles offer a unique advantage in timing precision. Frozen transfers require endometrial preparation through hormone protocols, which may not always mimic the natural receptivity window. For example, a 2021 study in *Fertility and Sterility* found that fresh transfers had a 40% implantation rate compared to 35% for frozen transfers, partly due to the ability to align embryo development with natural endometrial changes. However, fresh cycles carry a higher risk of cycle cancellation (5–10%) due to ovarian hyperstimulation syndrome (OHSS), particularly in younger patients (<35 years) with high AMH levels (>4 ng/mL).
Practical tips for optimizing timing include maintaining a consistent sleep schedule, as circadian rhythm disruptions can alter endometrial receptivity. Patients should avoid strenuous exercise 48 hours before and after transfer, as it may reduce uterine blood flow. Additionally, stress management techniques, such as mindfulness or yoga, can improve outcomes by stabilizing cortisol levels, which are known to impact implantation. For clinics, using time-lapse embryo monitoring systems can help select embryos with the highest developmental synchrony, further refining the timing of transfer.
In conclusion, the success of fresh, non-frozen embryo implantation hinges on precise timing that aligns the embryo’s developmental stage with the endometrium’s receptivity window. Clinicians must employ rigorous monitoring and individualized protocols to maximize implantation rates. Patients, meanwhile, can enhance outcomes through lifestyle adjustments that support uterine readiness. While fresh transfers offer timing advantages, they require careful candidate selection to avoid complications. Together, these strategies create a synergistic approach to achieving optimal implantation without freezing.
Freezing Cottage Cheese: A Guide to Preserving Freshness for Later Use
You may want to see also
Explore related products





![]()
Cost Comparison: Fresh vs. Frozen
Embryo transfer without freezing, often referred to as a fresh embryo transfer, is a viable option in assisted reproductive technology (ART). However, the decision between fresh and frozen embryos often hinges on cost, success rates, and individual medical circumstances. A cost comparison reveals nuanced financial implications that extend beyond the initial procedure, factoring in medication, monitoring, and potential repeat cycles.
Analytical Breakdown: Initial Costs and Hidden Expenses
Fresh embryo transfers typically incur higher upfront costs due to the need for ovarian stimulation and egg retrieval within the same cycle. This includes medications like gonadotropins (e.g., follicle-stimulating hormone, FSH) ranging from $3,000 to $5,000 per cycle, ultrasound monitoring ($500–$1,000), and the retrieval procedure itself ($3,000–$5,000). In contrast, frozen embryo transfers (FETs) bypass these steps, reducing costs by approximately 30–40% since they only involve thawing and transfer ($1,000–$3,000). However, FETs often require additional hormone medications (e.g., estrogen and progesterone) to prepare the uterus, adding $500–$1,000 per cycle.
Instructive Perspective: When to Choose Fresh or Frozen
Opt for a fresh transfer if your medical profile aligns with immediate implantation, such as in cases of normal hormone levels and uterine lining thickness. For patients with conditions like polycystic ovary syndrome (PCOS) or endometriosis, FETs may be more cost-effective due to the ability to optimize uterine conditions in a separate cycle. Always consult your fertility specialist to weigh the pros and cons based on age, ovarian reserve, and previous ART outcomes.
Comparative Insight: Long-Term Financial Considerations
While fresh transfers appear costlier initially, they may be more economical if successful on the first attempt. Frozen cycles, though cheaper per transfer, often require multiple attempts due to lower success rates in certain populations (e.g., women over 38). For instance, a single fresh cycle costing $15,000 might yield a live birth, whereas two FETs at $5,000 each would total $10,000 but with no guarantee of success. Insurance coverage also plays a critical role; some plans cover fresh cycles but not FETs, or vice versa.
Persuasive Argument: The Value of Flexibility
Frozen embryos offer flexibility in timing and planning, which can indirectly reduce costs by allowing patients to space out treatments or align them with financial readiness. For example, a patient can freeze embryos during a high-response stimulation cycle and use them later, avoiding the expense of repeat retrievals. This approach is particularly beneficial for those with unpredictable ovarian responses or those seeking to preserve fertility before medical treatments like chemotherapy.
Descriptive Takeaway: Real-World Scenarios
Consider a 32-year-old woman with regular cycles and a partner with normal sperm parameters. A fresh transfer might cost $12,000 but could result in pregnancy in one cycle. Conversely, a 40-year-old with diminished ovarian reserve might spend $8,000 on a frozen transfer but require three attempts, totaling $24,000. These scenarios underscore the importance of tailoring the choice to individual factors, balancing cost with the likelihood of success.
In summary, the cost comparison between fresh and frozen embryo transfers is not one-size-fits-all. It demands a personalized approach, factoring in medical history, age, and financial constraints. By understanding these nuances, patients can make informed decisions that optimize both outcomes and expenses.
Is Two-Year-Old Frozen Stew Beef Still Safe to Cook?
You may want to see also
Explore related products






![]()
Success Rates Without Freezing
Embryo transfer without prior freezing, known as fresh embryo transfer, remains a cornerstone of in vitro fertilization (IVR) protocols, particularly for patients with favorable prognoses. Success rates for fresh transfers are influenced by factors such as maternal age, embryo quality, and uterine receptivity. For women under 35, live birth rates from fresh transfers average 40-50%, according to data from the Society for Assisted Reproductive Technology (SART). This drops to 30-35% for women aged 35-37 and further declines with advancing age. Optimal outcomes are associated with single embryo transfers of high-quality blastocysts, which reduce multiple pregnancy risks while maintaining robust implantation rates.
Fresh transfers offer logistical advantages, including shorter treatment cycles and reduced costs compared to frozen embryo transfers (FET). However, they are not universally applicable. Patients with conditions like polycystic ovary syndrome (PCOS) or those undergoing preimplantation genetic testing (PGT) often require freezing to mitigate risks of ovarian hyperstimulation syndrome (OHSS) or to await genetic results. Clinicians must weigh these factors when deciding between fresh and frozen approaches, ensuring the chosen method aligns with individual patient needs and safety profiles.
A critical determinant of success in fresh transfers is the synchronization of embryo development with endometrial receptivity. Protocols such as natural cycle transfers or mild stimulation cycles aim to achieve this alignment, though they may yield fewer embryos for transfer. For instance, natural cycle transfers, which rely on a single mature follicle, report implantation rates of 15-20% per cycle but offer a more physiological environment for embryo development. Conversely, antagonist protocols, which suppress premature ovulation while stimulating multiple follicles, can produce higher embryo yields with implantation rates approaching 30-35%.
Despite their benefits, fresh transfers are not without limitations. The absence of a freeze-thaw process eliminates the ability to assess embryo survival post-thaw, a step that can serve as a quality control measure in FET cycles. Additionally, fresh transfers may be contraindicated in cases where the endometrial lining is suboptimal, as measured by ultrasound assessments or biomarker analysis. In such scenarios, delaying transfer and opting for a frozen cycle may improve outcomes. Patients and providers must collaborate to determine the most appropriate timing and method for embryo transfer, balancing success rates with safety and individual circumstances.
Practical considerations for maximizing success in fresh transfers include lifestyle modifications such as maintaining a healthy BMI, avoiding smoking, and adhering to prescribed medications like progesterone supplementation. Progesterone dosing typically ranges from 200-400 mg daily, administered via vaginal suppositories or intramuscular injections, to support endometrial thickening and vascularization. Monitoring through serial hormone assays and ultrasounds ensures that the endometrium remains receptive during the critical implantation window. By addressing these factors, fresh embryo transfers can remain a viable and effective option for achieving successful pregnancies without the need for freezing.
Chest Freezer Power Consumption: Understanding Energy Usage and Costs
You may want to see also
Frequently asked questions
Yes, embryos can be used without freezing in a process called fresh embryo transfer, where they are transferred to the uterus shortly after fertilization, typically within 1-5 days.
Fresh embryo transfer can be equally effective as frozen embryo transfer, depending on individual factors such as the patient’s health, embryo quality, and the specific circumstances of the fertility treatment.
Fresh embryo transfer is often preferred when there are no medical reasons to delay implantation, when the uterine lining is optimally prepared, or when the patient wishes to avoid the costs and risks associated with embryo freezing.
The risks of fresh embryo transfer are generally minimal but may include ovarian hyperstimulation syndrome (OHSS) if fertility medications were used, or a slightly higher chance of cycle cancellation if the uterine lining is not ready.
Embryos can be cultured in a laboratory for a short period (typically up to 5-6 days) without freezing, but long-term storage requires cryopreservation to preserve their viability.